Abstract
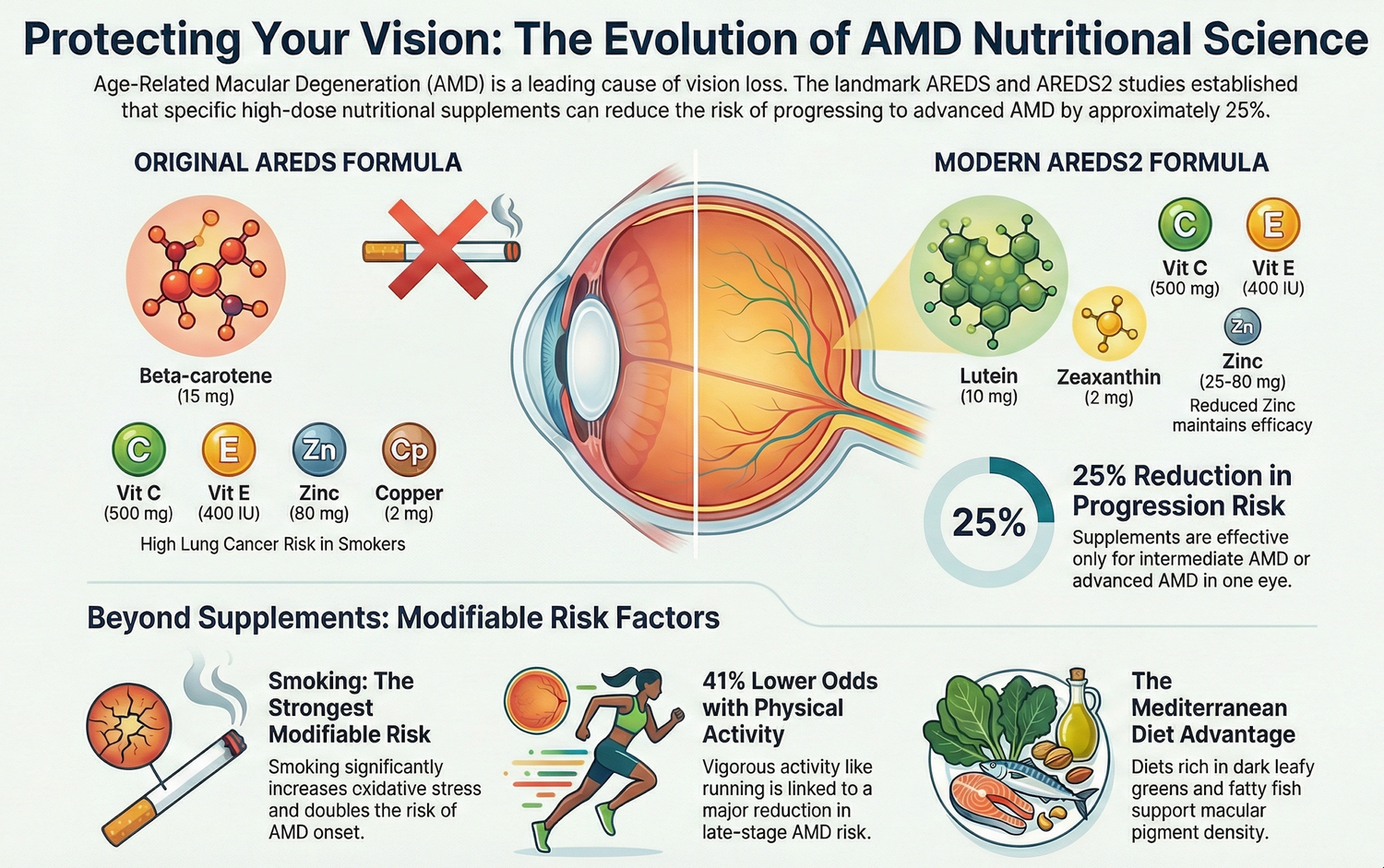
The original Age-Related Eye Disease Study (AREDS) established that high-dose antioxidant vitamins (vitamin C, vitamin E, β‑carotene) plus zinc and copper reduced the 5‑year risk of progression to advanced age-related macular degeneration (AMD) by about 25% in individuals with intermediate AMD or advanced AMD in one eye.(1,2) However, safety concerns regarding β‑carotene in smokers, questions about the optimal zinc dose, and emerging evidence for macular carotenoids and omega‑3 fatty acids prompted the Age-Related Eye Disease Study 2 (AREDS2), which tested refinements to the original formulation.(3,4) AREDS2 evaluated the addition of lutein/zeaxanthin and docosahexaenoic acid (DHA)/eicosapentaenoic acid (EPA), the removal of β‑carotene, and reduction of zinc dose, in a multicentre randomized trial of 4,203 participants at high risk of advanced AMD.(3,4)
AREDS2 demonstrated that adding lutein/zeaxanthin and omega‑3 fatty acids to the original formula did not further reduce progression risk overall, but substituting lutein/zeaxanthin for β‑carotene provided at least equivalent efficacy and improved safety, especially regarding lung cancer risk in former smokers.(3–5) Long-term follow-up over 10 years confirmed a persistent beneficial association of lutein/zeaxanthin with reduced progression to late AMD and showed that β‑carotene supplementation nearly doubled lung cancer risk, whereas lutein/zeaxanthin did not increase cancer incidence.(5) Analyses also indicated that lowering zinc from 80 mg to 25 mg did not materially affect efficacy, though current AREDS2-type products commonly retain 80 mg due to historical precedent and regulatory considerations.(3–5)
As a result, contemporary “AREDS2” supplements typically contain vitamin C (500 mg), vitamin E (400 IU), zinc (usually 80 mg zinc oxide), copper (2 mg cupric oxide), lutein (10 mg), and zeaxanthin (2 mg), without β‑carotene and without omega‑3 fatty acids.(3–5,7) This article reviews the rationale and design of AREDS and AREDS2, highlights key differences in formulations and outcomes, discusses implications for clinical practice and patient selection, and summarizes remaining questions regarding optimal dosing, duration of therapy, and interaction with diet and genetics.
Introduction
Oxidative stress and chronic inflammation play central roles in the pathogenesis of age-related macular degeneration, particularly at the level of the retinal pigment epithelium and photoreceptors.(1,8) Early epidemiologic studies suggested that higher dietary intake of antioxidant vitamins and zinc was associated with lower AMD risk, providing the rationale for formal trials of nutritional supplementation.(1,8,9) The National Eye Institute initiated the AREDS trial in the early 1990s to evaluate whether high-dose antioxidant vitamins and zinc could slow progression to advanced AMD and cataract.(1,2)
AREDS showed that a specific formulation of antioxidants plus zinc reduced the risk of progressing to advanced AMD in high-risk individuals, establishing a new standard of care for patients with intermediate disease.(1,2) However, several limitations emerged. β‑carotene was later linked to increased lung cancer risk in current and former smokers; the high zinc dose raised tolerability and safety questions; and the formulation did not include lutein, zeaxanthin, or omega‑3 fatty acids, which accumulating evidence suggested may benefit macular health.(3,4,8–10)
AREDS2 was therefore designed to refine the original formula by testing additional or alternative nutrients while preserving the proven core of antioxidants and zinc.(3,4) Understanding what changed between AREDS and AREDS2—and why—is critical for clinicians recommending supplements and for patients selecting evidence-based products.
Mechanistic Rationale for Key Nutrients
Oxidative Stress, Antioxidants, and Zinc
The macula is exposed to high metabolic demand, oxygen tension, and light, making it susceptible to oxidative damage.(8,9) Vitamin C, vitamin E, and β‑carotene function as antioxidants that scavenge reactive oxygen species and protect cellular lipids, proteins, and DNA.(1,8,9) Zinc is a cofactor for numerous enzymes, including antioxidant enzymes such as superoxide dismutase, and may stabilize cell membranes and modulate immune function.(1,8,9)
The AREDS formulation—vitamin C 500 mg, vitamin E 400 IU, β‑carotene 15 mg, zinc oxide 80 mg, and cupric oxide 2 mg—was selected based on prior observational and mechanistic evidence that high-dose antioxidant and zinc supplementation could counteract oxidative damage and slow AMD progression.(1,2,9) Copper was included to reduce the risk of copper deficiency anemia associated with high-dose zinc.(1,2)
Macular Carotenoids: Lutein and Zeaxanthin
Lutein and zeaxanthin are xanthophyll carotenoids concentrated in the macular pigment, where they filter short-wavelength blue light and possess antioxidant properties.(8,9,11) Higher dietary intake and higher macular pigment optical density have been associated with reduced AMD prevalence and slower progression in some observational studies.(11,12) Unlike β‑carotene, these carotenoids were not associated with increased lung cancer risk and could directly augment macular pigment.
AREDS did not include lutein or zeaxanthin because their importance was less well-recognized at the time of trial design. AREDS2 specifically tested whether adding these carotenoids to, or substituting them for, β‑carotene would improve outcomes.(3,4,11–13)
Omega‑3 Fatty Acids: DHA and EPA
Docosahexaenoic acid (DHA) is abundant in photoreceptor outer segment membranes, and both DHA and EPA have anti-inflammatory and neuroprotective properties.(8,10) Observational studies suggested that higher dietary intake of marine omega‑3 fatty acids was associated with lower risk of AMD development or progression.(10,14) AREDS2 therefore evaluated whether supplementation with DHA (350 mg) and EPA (650 mg) could enhance the protective effect of the AREDS formulation.(3,4,10,14)
AREDS: Design, Formulation, and Key Findings
Study Design and Population
AREDS enrolled 4,757 participants aged 55–80 years at 11 U.S. clinical centres.(1,2) Participants were categorized into four AMD severity categories based on fundus photographs, from no AMD to advanced disease.(1,2) The trial had a factorial design evaluating the effect of antioxidant vitamins, zinc, the combination, or placebo on progression to advanced AMD and cataract.(1,2)
The primary AMD outcome was progression to advanced AMD (neovascular AMD or central geographic atrophy) in at least one eye over a median follow-up of 6.3 years.(1,2)
AREDS Formulation
The AREDS supplement contained: vitamin C 500 mg, vitamin E 400 IU, β‑carotene 15 mg, zinc oxide 80 mg, and cupric oxide 2 mg daily.(1,2) Participants were randomised to antioxidants alone, zinc alone, antioxidants plus zinc (the full formulation), or placebo.
Main Results
In participants with intermediate AMD (extensive drusen or non-central geographic atrophy) or advanced AMD in one eye (categories 3 and 4), the combination of antioxidants plus zinc reduced the 5‑year risk of progression to advanced AMD by about 25% relative to placebo.(1,2) The absolute risk reduction was 7.6%, corresponding to a number needed to treat of approximately 13 to prevent one case of advanced AMD over 5 years.(1,2)
The formulation did not significantly affect the incidence or progression of cataract.(1,2) Subgroup analyses suggested that zinc-containing regimens were primarily responsible for the protective effect, with antioxidants alone conferring less benefit.(1,2)
AREDS2: Rationale, Modifications, and Primary Outcomes
Goals and Design
AREDS2 sought to refine the AREDS formulation by addressing three main questions:(3,4)
- Does adding lutein/zeaxanthin and/or DHA/EPA to the original AREDS formulation further reduce progression to advanced AMD?
- Can β‑carotene be safely removed and replaced with lutein/zeaxanthin without loss of efficacy, reducing lung cancer risk in former smokers?
- Does lowering the zinc dose from 80 mg to 25 mg maintain efficacy while improving tolerability?
AREDS2 randomized 4,203 participants aged 50–85 years with bilateral large drusen or large drusen in one eye and advanced AMD in the fellow eye.(3,4) All participants received some form of the original AREDS formulation; the primary randomization concerned the addition of lutein/zeaxanthin, DHA/EPA, both, or placebo, while a secondary randomization examined β‑carotene vs no β‑carotene and high vs low zinc.(3,4)
Modifications Tested
The key nutrient modifications were:(3,4)
- Lutein 10 mg and zeaxanthin 2 mg (added or substituted for β‑carotene).
- DHA 350 mg and EPA 650 mg.
- Removal of β‑carotene.
- Reduction of zinc from 80 mg to 25 mg.
Primary Outcomes
The primary result was that adding lutein/zeaxanthin and/or DHA/EPA to the original AREDS formulation did not significantly further reduce the overall risk of progression to advanced AMD beyond the benefit conferred by the base formulation.(3,4) However, secondary analyses and long-term follow-up revealed important nuances regarding carotenoid substitution and safety.
What AREDS2 Changed and Why It Matters
Replacement of β‑Carotene with Lutein/Zeaxanthin
In AREDS2, participants who received lutein/zeaxanthin instead of β‑carotene had a modestly reduced risk of progression to advanced AMD compared with those receiving β‑carotene, particularly among participants with low dietary intake of lutein/zeaxanthin.(3,4,12,13) Importantly, β‑carotene supplementation was associated with approximately double the risk of lung cancer, predominantly in former smokers, whereas lutein/zeaxanthin were not associated with increased cancer risk.(3–5,13)
A 10‑year follow-up of the AREDS2 cohort confirmed a persistent beneficial association of lutein/zeaxanthin with reduced progression to late AMD and reaffirmed the increased lung cancer risk with β‑carotene.(5,15) These findings support replacing β‑carotene with lutein/zeaxanthin in AMD supplements, especially for current or former smokers.
Omega‑3 Fatty Acids Did Not Improve Outcomes
Contrary to expectations based on observational data, supplementation with DHA/EPA did not significantly reduce progression to advanced AMD when added to the AREDS formulation.(3,4,10,14) Reasons may include high baseline dietary omega‑3 intake in the study population, limited dose or duration, or differences between long-term dietary patterns and supplementation. As a result, omega‑3 fatty acids are not included in the standard AREDS2 supplement, though diets rich in oily fish remain generally recommended for cardiovascular and potential ocular benefits.(8,10,14)
Zinc Dose Reduction: Efficacy vs Safety
AREDS2 compared 80 mg versus 25 mg zinc oxide and found no statistically significant difference in AMD progression, suggesting that lower zinc doses may be adequate.(3,4,5) However, the trial was not primarily powered to detect small differences between zinc doses, and regulatory considerations meant that many commercial formulations retained the 80 mg dose.(3–5,7,15) High-dose zinc can cause gastrointestinal side effects and may affect copper and iron metabolism, so some clinicians prefer lower-zinc formulations, particularly in patients with comorbidities.(3,4,7,9)
Clinical Practice Implications
Who Benefits from AREDS2 Supplements?
Both AREDS and AREDS2 found that benefits are largely confined to individuals with intermediate AMD or advanced AMD in one eye; supplements did not prevent AMD onset in people with minimal or no disease.(1–4) Current guidelines therefore recommend AREDS2-type supplements for patients with:(1–4,7,9)
- Intermediate AMD in one or both eyes (numerous medium drusen or at least one large druse).
- Advanced AMD (geographic atrophy involving the centre or neovascular AMD) in one eye and early or intermediate AMD in the fellow eye.
Supplements have not been shown to benefit patients with no AMD or very early changes and are not indicated for these groups.(1–4,7)
Current Standard Formulation
Based on AREDS2 data and safety considerations, the commonly recommended “AREDS2” supplement contains:(3–5,7)
- Vitamin C 500 mg
- Vitamin E 400 IU
- Zinc (usually 80 mg zinc oxide, though some products use 25–40 mg)
- Copper 2 mg (as cupric oxide)
- Lutein 10 mg
- Zeaxanthin 2 mg
β‑carotene is omitted, and omega‑3 fatty acids are not part of the core formula. Patients who smoke or have a history of smoking should specifically avoid β‑carotene-containing products due to lung cancer risk.(3–5,13,15)
Individualization and Safety Considerations
Clinicians should consider dietary intake, smoking history, comorbidities, and concomitant medications when recommending supplements.(7,9,15,16) Key points include:
- Avoid β‑carotene in current or former smokers due to increased lung cancer risk.(3–5,13,15)
- Monitor for gastrointestinal intolerance or potential interactions in patients on high-dose zinc; lower-zinc formulations may be reasonable where tolerated.(3–5,9,16)
- Reinforce that supplements are adjunctive to, not replacements for, regular ophthalmic monitoring, smoking cessation, blood pressure and lipid management, and a balanced diet rich in leafy greens and fish.(8–10,14,16)
Emerging Research Directions
Long-Term Outcomes and Real-World Use
The 10‑year AREDS2 follow-up showed that the beneficial association of lutein/zeaxanthin with reduced AMD progression persisted over a decade and that AREDS2 supplements were generally safe for long-term use.(5,15) Ongoing observational studies are examining real-world adherence, interactions with genetic risk factors (for example CFH and ARMS2 variants), and combined use with other therapies such as complement inhibitors.(15–17)
Genetic Stratification and Precision Nutrition
Preliminary analyses suggest that genetic variants in complement and lipid metabolism genes may influence response to antioxidant and zinc supplementation, though findings are not yet sufficiently consistent to guide genotype-specific recommendations.(16,17) Future research may clarify whether certain genotypes benefit more from specific nutrient combinations or doses, moving toward precision nutrition for AMD.
Beyond AREDS2: Additional Nutrients and Formulations
Interest continues in additional nutrients such as meso‑zeaxanthin, resveratrol, and novel antioxidants, but robust randomized trials comparable to AREDS/AREDS2 are lacking.(11,12,18) For now, AREDS2 remains the most well-validated formulation, and clinicians should be cautious about extrapolating benefits from untested combinations.
Conclusion
The evolution from AREDS to AREDS2 reflects both advances in AMD pathophysiology and a commitment to refining therapy based on rigorous clinical evidence. The original AREDS formulation demonstrated that high-dose antioxidant vitamins plus zinc can reduce progression to advanced AMD in high-risk individuals, establishing nutritional supplementation as a cornerstone of care.(1,2) AREDS2 confirmed that the core protective effect is maintained when β‑carotene is removed and lutein/zeaxanthin are added, while omega‑3 fatty acid supplementation does not confer additional benefit in this context.(3–5)
Critically, AREDS2 showed that replacing β‑carotene with lutein/zeaxanthin preserves or slightly enhances efficacy and markedly improves safety, particularly in former smokers, and that lower zinc doses may be adequate for many patients.(3–5,13,15) The resulting AREDS2-type formulation—vitamin C, vitamin E, zinc, copper, lutein, and zeaxanthin—is now the recommended standard for patients with intermediate AMD or advanced AMD in one eye.
Future work will focus on optimizing zinc dosing, clarifying genetic modifiers of response, and integrating AREDS2 supplementation with emerging therapies such as complement inhibitors and ferroptosis-targeted approaches. For now, consistent use of well-validated AREDS2 supplements, alongside lifestyle modifications and regular ophthalmic care, remains an important strategy for slowing progression in patients at risk of advanced AMD.
This article is for educational purposes only and reflects current scientific literature at the time of writing.
References
- Age-Related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch Ophthalmol. 2001;119(10):1417–1436. https://pubmed.ncbi.nlm.nih.gov/11594942[pmc.ncbi.nlm.nih]
- Age-Related Eye Disease Study Research Group. A simplified severity scale for age-related macular degeneration: AREDS report no. 18. Arch Ophthalmol. 2005;123(11):1570–1574. https://pmc.ncbi.nlm.nih.gov/articles/PMC3485447/[pmc.ncbi.nlm.nih]
- Age-Related Eye Disease Study 2 Research Group. Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: the Age-Related Eye Disease Study 2 (AREDS2) randomized clinical trial. JAMA. 2013;309(19):2005–2015. https://jamanetwork.com/journals/jama/fullarticle/1684847[jamanetwork]
- Chew EY, SanGiovanni JP, Ferris FL, et al. The Age-Related Eye Disease Study 2 (AREDS2): rationale and study design. Ophthalmology. 2012;119(11):2282–2289. https://pmc.ncbi.nlm.nih.gov/articles/PMC3485447/[pmc.ncbi.nlm.nih]
- Chew EY, Clemons TE, Agrón E, et al. Long-term outcomes of adding lutein/zeaxanthin and ω‑3 fatty acids to the AREDS supplements on age-related macular degeneration progression and lung cancer: AREDS2 10‑year follow-up. JAMA Ophthalmol. 2022;140(8):834–843. https://jamanetwork.com/journals/jamaophthalmology/fullarticle/2792855[jamanetwork]
- National Eye Institute. AREDS/AREDS2 Frequently Asked Questions. National Institutes of Health. 2020. https://www.nei.nih.gov/eye-health/clinical-trials/areds-areds2-faq[nei.nih]
- Macular Degeneration Association. AREDS and AREDS2 supplements for macular degeneration. 2025. https://maculardegeneration.net/areds-vs-areds2[maculardegeneration]
- Jarrett SG, Boulton ME. Consequences of oxidative stress in age-related macular degeneration. Mol Aspects Med. 2012;33(4):399–417. https://pmc.ncbi.nlm.nih.gov/articles/PMC3392472/[ncbi.nlm.nih]
- Seddon JM, Ajani UA, Sperduto RD, et al. Dietary carotenoids, vitamins A, C, and E, and advanced age-related macular degeneration. JAMA. 1994;272(18):1413–1420. https://pubmed.ncbi.nlm.nih.gov/7933422[pmc.ncbi.nlm.nih]
- SanGiovanni JP, Chew EY, Clemons TE, et al. The relationship of dietary omega‑3 long-chain polyunsaturated fatty acid intake with incident age-related macular degeneration. Am J Clin Nutr. 2008;88(2):398–406. https://pmc.ncbi.nlm.nih.gov/articles/PMC6774801/[pmc.ncbi.nlm.nih]
- Ma L, Dou HL, Wu YQ, et al. Lutein and zeaxanthin and their roles in age-related macular degeneration. J Ophthalmol. 2013;2013:120864. https://pmc.ncbi.nlm.nih.gov/articles/PMC6774801/[pmc.ncbi.nlm.nih]
- Bernstein PS, Li B, Vachali PP, et al. Lutein, zeaxanthin, and meso‑zeaxanthin: the basic and clinical science underlying carotenoid-based nutritional interventions for retinal disease. Prog Retin Eye Res. 2016;50:34–66. https://pmc.ncbi.nlm.nih.gov/articles/PMC6774801/[pmc.ncbi.nlm.nih]
- Chew EY, Clemons TE, Sangiovanni JP, et al. Secondary analyses of the effects of lutein/zeaxanthin on age-related macular degeneration progression: AREDS2 report no. 3. JAMA Ophthalmol. 2014;132(2):142–149. https://jamanetwork.com/journals/jamaophthalmology/fullarticle/1792910[jamanetwork]
- Christen WG, Schaumberg DA, Glynn RJ, Buring JE. Dietary omega‑3 fatty acid and fish intake and incident age-related macular degeneration in women. Arch Ophthalmol. 2011;129(7):921–929. https://pmc.ncbi.nlm.nih.gov/articles/PMC6774801/[pmc.ncbi.nlm.nih]
- BrightFocus Foundation. New study confirms the efficacy of AREDS2 eye vitamin supplement for slowing age-related macular degeneration. 2025. https://www.brightfocus.org/resource/new-study-confirms-the-efficacy-of-areds2-eye-vitamin-supplement-for-slowing-age-related-macular-degeneration[brightfocus]
- Seddon JM, Reynolds R, Yu Y, Daly MJ, Rosner B. Risk models for progression to advanced AMD using demographic, environmental, genetic, and ocular factors. Ophthalmology. 2011;118(11):2203–2211. https://pmc.ncbi.nlm.nih.gov/articles/PMC8195907/[pmc.ncbi.nlm.nih]
- Awh CC, Lane AM, Hawken S, Zanke B, Kim IK. CFH and ARMS2 genetic polymorphisms predict response to antioxidants and zinc in AMD: independent confirmation and extended analysis of the AREDS report no. 38. Ophthalmology. 2013;120(11):2317–2323. https://pmc.ncbi.nlm.nih.gov/articles/PMC8195907/[pmc.ncbi.nlm.nih]
- Beatty S, Chakravarthy U, Nolan JM, et al. Secondary outcomes in a clinical trial of macular pigment supplementation in patients with age-related macular degeneration. Invest Ophthalmol Vis Sci. 2013;54(7):4561–4570. https://pmc.ncbi.nlm.nih.gov/articles/PMC6774801/[pmc.ncbi.nlm.nih]
{kind=link}
Leave a comment
This site is protected by hCaptcha and the hCaptcha Privacy Policy and Terms of Service apply.