Age-Related Macular Degeneration (AMD): Pathophysiology, Risk Factors, Nutritional Science, and Emerging Research (2026 Scientific Review)
What is Age-Related Macular Degeneration?
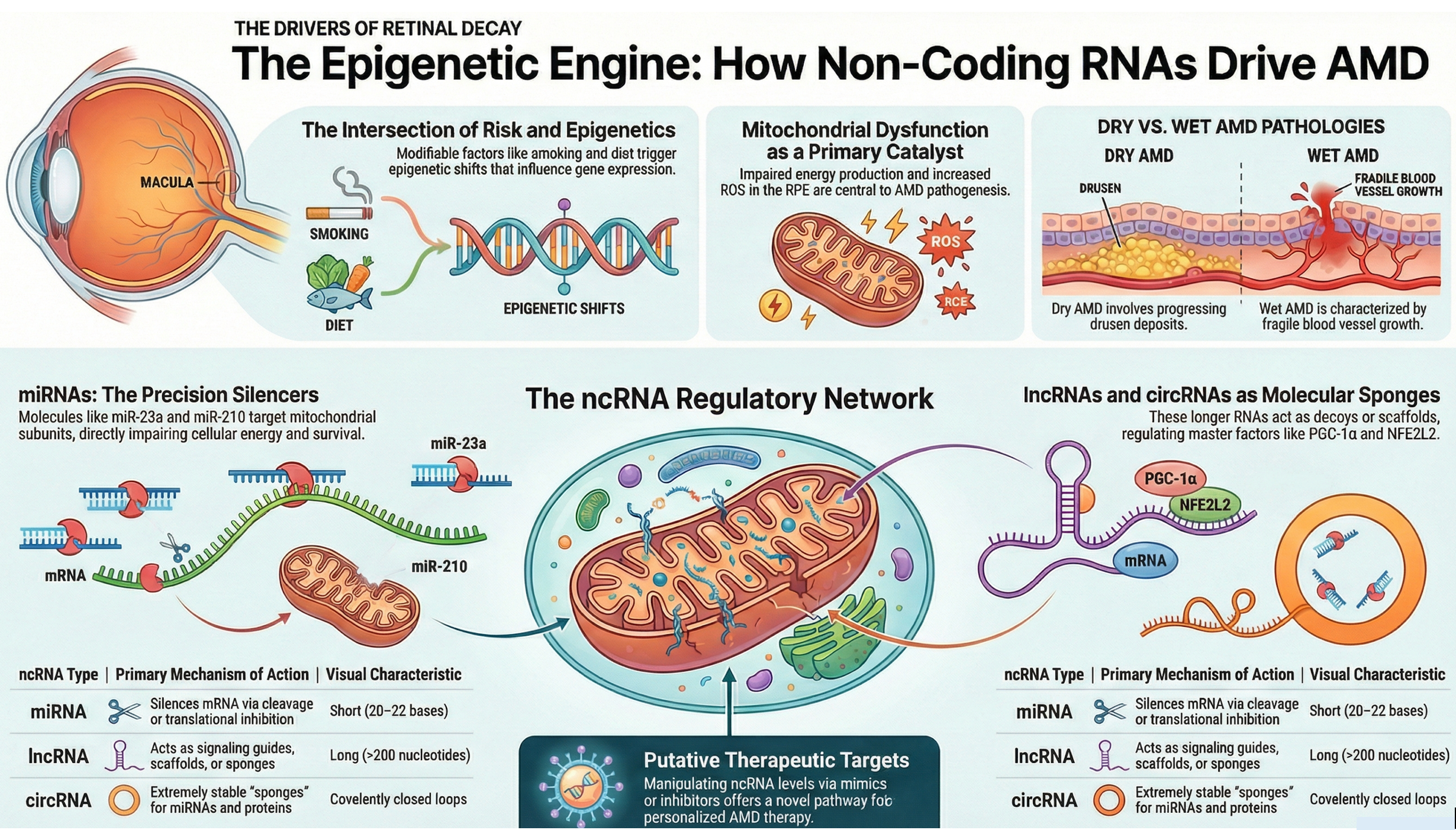
Age-related macular degeneration (AMD) is a progressive retinal disorder affecting the macula, the central region of the retina responsible for sharp vision. It is characterized by dysfunction of the retinal pigment epithelium (RPE), accumulation of drusen beneath Bruch’s membrane, oxidative injury, chronic inflammation, lipid dysregulation, and in advanced stages, geographic atrophy or choroidal neovascularization [1–4].
AMD is broadly classified into:
- Dry (atrophic) AMD
- Wet (neovascular) AMD
1. Epidemiology and Clinical Overview
AMD is a leading cause of irreversible vision loss among individuals over 50 years of age in developed countries [1]. Globally, prevalence is projected to reach nearly 288 million by 2040 [1].
Clinical progression includes:
- Early AMD: Presence of drusen
- Intermediate AMD: Large drusen, pigmentary changes
- Advanced AMD:
- Geographic atrophy (dry)
- Neovascular AMD (wet)
2. Pathophysiology of AMD
Oxidative Stress
The retina has one of the highest metabolic demands in the body. Chronic oxidative stress leads to lipid peroxidation, mitochondrial dysfunction, and RPE injury [2,5].
Reactive oxygen species (ROS) damage photoreceptors and contribute to drusen formation [2].
Chronic Inflammation
AMD is strongly associated with complement system dysregulation, particularly variants in complement factor H (CFH) [3].
Chronic low-grade inflammation contributes to structural retinal damage [3].
Lipid Dysregulation
Drusen contain lipids, cholesterol esters, and apolipoproteins, linking AMD to altered lipid metabolism [4].
Bruch’s membrane thickening impairs nutrient exchange between the choroid and retina [4].
Iron Homeostasis and Ferroptosis
Iron accumulation in the retina contributes to oxidative injury and ferroptosis, a form of iron-dependent cell death [6,7].
Ferroptotic pathways are increasingly implicated in geographic atrophy progression [7].
RPE Dysfunction
The retinal pigment epithelium maintains photoreceptor survival, phagocytoses outer segments, and regulates oxidative balance. RPE degeneration is central to AMD pathogenesis [2].
3. Genetic and Molecular Influences
Genome-wide association studies have identified multiple loci associated with AMD, including:
- CFH
- ARMS2/HTRA1
- C3
- C2
These genes influence complement activation and inflammatory responses [3].
Environmental factors such as smoking may interact with genetic susceptibility.
4. Modifiable Risk Factors
Smoking
Smoking significantly increases AMD risk through oxidative stress and vascular impairment [8].
Cardiovascular Health
Hypertension and atherosclerosis are associated with AMD progression [9].
Diet and Obesity
High glycemic index diets and obesity correlate with increased AMD risk [10].
Physical Activity
Regular physical activity is associated with lower incidence of early AMD [11].
5. Nutritional Science and Supplement Research
AREDS and AREDS2
The Age-Related Eye Disease Study (AREDS) demonstrated that specific antioxidant combinations reduced progression to advanced AMD by approximately 25% in high-risk individuals [12].
AREDS2 replaced beta-carotene with lutein and zeaxanthin due to lung cancer risk in smokers [13].
Lutein and Zeaxanthin
These carotenoids accumulate in the macula and may improve macular pigment density [13].
Vitamin D
Observational studies suggest associations between low vitamin D and AMD, though causality remains under investigation [14].
Resveratrol
Resveratrol demonstrates anti-inflammatory and antioxidant properties in retinal models [15].
Saffron Research
Clinical studies suggest saffron supplementation may improve retinal function and macular sensitivity in early AMD [16,17].
6. Emerging Research Directions
- Complement inhibitors for geographic atrophy
- Iron chelation strategies
- Ferroptosis modulation
- Regenerative retinal therapies
- RPE cell replacement
Research continues to explore mechanisms linking oxidative stress, lipid metabolism, and inflammation [6,7].
Key Scientific Takeaways
- AMD is driven by oxidative stress, inflammation, lipid dysregulation, and iron imbalance.
- RPE dysfunction is central to disease progression.
- Genetic predisposition influences complement pathway activation.
- Smoking and metabolic health significantly affect risk.
- AREDS-based nutritional interventions reduce progression in high-risk individuals.
- Ferroptosis is an emerging therapeutic target.
Frequently Asked Questions (Scientific)
Can AMD be reversed?
Currently, advanced AMD cannot be reversed, but progression may be slowed through risk factor modification and evidence-based nutritional strategies [12].
What nutrients have the strongest clinical evidence?
AREDS/AREDS2 formulations including vitamins C, E, zinc, lutein, and zeaxanthin have the strongest evidence for slowing progression in high-risk individuals [12,13].
Is iron involved in AMD?
Emerging research suggests iron accumulation and ferroptosis may contribute to retinal degeneration [6,7].
What is geographic atrophy?
Geographic atrophy is the advanced atrophic form of dry AMD characterized by progressive loss of RPE and photoreceptors.
Download this article in PDF format by clicking here...
References
- Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration. Lancet Glob Health. 2014;2(2):e106–e116.
https://pubmed.ncbi.nlm.nih.gov/25104651/ - Beatty S, Koh H, Phil M, et al. The role of oxidative stress in the pathogenesis of age-related macular degeneration. Surv Ophthalmol. 2000;45(2):115–134.
https://pubmed.ncbi.nlm.nih.gov/11033038/ - Haines JL, Hauser MA, Schmidt S, et al. Complement factor H variant increases AMD risk. Science. 2005;308(5720):419–421.
https://pubmed.ncbi.nlm.nih.gov/15761120/ - Curcio CA, Johnson M, Huang JD, Rudolf M. Aging, lipids, and AMD. Prog Retin Eye Res. 2009;28(6):393–422.
https://pubmed.ncbi.nlm.nih.gov/19698799/ - Jarrett SG, Boulton ME. Consequences of oxidative stress in AMD. Mol Aspects Med. 2012;33(4):399–417.
https://pubmed.ncbi.nlm.nih.gov/22510306/ - Ueda K, et al. Iron accumulation and oxidative damage in AMD. Investig Ophthalmol Vis Sci. 1998.
https://pubmed.ncbi.nlm.nih.gov/9497478/ - Tang D, Kroemer G. Ferroptosis in retinal degeneration. Cell Death Differ. 2020.
https://pubmed.ncbi.nlm.nih.gov/32066980/ - Thornton J, Edwards R, Mitchell P, et al. Smoking and AMD risk. Eye. 2005.
https://pubmed.ncbi.nlm.nih.gov/15688054/ - Klein R, Klein BEK, Knudtson MD, et al. Cardiovascular risk factors and AMD. Ophthalmology. 2003.
https://pubmed.ncbi.nlm.nih.gov/14597581/ - Chiu CJ, Taylor A. Dietary glycemic index and AMD. Am J Clin Nutr. 2011.
https://pubmed.ncbi.nlm.nih.gov/21346088/ - Knudtson MD, Klein R, Klein BEK. Physical activity and AMD. Arch Ophthalmol. 2006.
https://pubmed.ncbi.nlm.nih.gov/17000949/ - AREDS Research Group. A randomized, placebo-controlled trial of high-dose supplementation. Arch Ophthalmol. 2001.
https://pubmed.ncbi.nlm.nih.gov/11594942/ - AREDS2 Research Group. Lutein/zeaxanthin and omega-3 fatty acids. JAMA. 2013.
https://pubmed.ncbi.nlm.nih.gov/23644932/ - Millen AE, et al. Vitamin D status and AMD. Arch Ophthalmol. 2011.
https://pubmed.ncbi.nlm.nih.gov/21825180/ - Kubota S, et al. Resveratrol and retinal protection. Mol Vis. 2010.
https://pubmed.ncbi.nlm.nih.gov/20431728/ - Falsini B, et al. Influence of saffron supplementation on retinal function. Invest Ophthalmol Vis Sci. 2010.
https://pubmed.ncbi.nlm.nih.gov/20071673/ - Piccardi M, et al. Saffron in early AMD. Evid Based Complement Alternat Med. 2012.
https://pubmed.ncbi.nlm.nih.gov/22701387/
{kind=link}
Leave a comment
This site is protected by hCaptcha and the hCaptcha Privacy Policy and Terms of Service apply.