1. Introduction: The Epidemiological and Clinical Imperative
Age-related macular degeneration (AMD) stands as the preeminent cause of irreversible blindness and visual impairment in the developed world, presenting a public health challenge of escalating magnitude. As global demographics shift towards an aging population, the prevalence of AMD is projected to surge, with estimates suggesting that the number of affected individuals will rise from approximately 200 million today to 288 million by the year 2040. This trajectory threatens to overwhelm healthcare infrastructures, necessitating a paradigm shift from a purely reactive, treatment-based model to one grounded in proactive prevention and risk mitigation.

For the past two decades, the management of AMD has been bifurcated. The neovascular (or "wet") form of the disease, characterized by choroidal neovascularization, has seen revolutionary advances with the advent of anti-vascular endothelial growth factor (anti-VEGF) therapies. These agents have transformed a once rapidly blinding condition into a manageable chronic disease for many. However, the non-neovascular (or "dry") form, particularly its advanced stage known as geographic atrophy (GA), has historically lacked effective pharmacological interventions. Even with the recent emergence of complement inhibitors, the therapeutic landscape for dry AMD remains limited, with treatments primarily focusing on slowing lesion growth rather than restoring vision. Furthermore, the burden of intravitreal injections for wet AMD places a colossal strain on patients, caregivers, and healthcare payers.
In this context, lifestyle modification has emerged not merely as an adjunct recommendation but as a central therapeutic pillar. A growing body of rigorous epidemiological evidence indicates that modifiable lifestyle factors—specifically smoking cessation, dietary adherence to Mediterranean patterns, physical activity, and targeted nutritional supplementation—can dramatically alter the natural history of the disease. Systematic reviews suggest that up to 60% of advanced AMD incidence is attributable to modifiable factors. More strikingly, adherence to a combination of healthy behaviors has been shown to reduce the risk of disease progression by nearly half, a magnitude of effect that rivals or exceeds many pharmacological agents currently in development.

However, the efficacy of lifestyle modification is contingent upon a critical, often overlooked variable: adherence. Unlike a surgical intervention or a clinician-administered injection, lifestyle modification requires sustained, daily engagement from the patient. "Adherence" in this context is defined not as a binary state of compliance but as a continuous variable reflecting the consistency, duration, and intensity of behavioral change. The gap between the theoretical efficacy of lifestyle changes (observed in controlled environments or high-adherence cohorts) and the real-world effectiveness (limited by socioeconomic, psychological, and systemic barriers) is the "adherence gap." Bridging this gap is the next frontier in ophthalmic epidemiology and public health.

This report provides an exhaustive analysis of the scientific literature regarding the importance of adherence to lifestyle behaviors in AMD. It moves beyond the simple identification of risk factors to explore the dose-response relationships of adherence, the complex interplay between genetics and lifestyle, the psychological frameworks underpinning patient behavior, and the emerging interventions—such as health coaching and digital health technologies—designed to optimize adherence. Furthermore, it examines the economic implications of adherence, modeling the potential cost savings associated with preventing the transition to late-stage disease.

2. Pathophysiological Mechanisms: Why Adherence Matters
To appreciate the criticality of adherence, one must first understand the biological vulnerability of the macula and how inconsistent lifestyle behaviors exacerbate pathological processes. The retina is a tissue of paradoxes; it requires high oxygen levels to function yet is extremely susceptible to oxidative damage. The photoreceptors and the retinal pigment epithelium (RPE) operate under a constant barrage of focused light and high metabolic demand, creating a potent pro-oxidative environment.
2.1 Oxidative Stress and the Cumulative Debt of Non-Adherence
Oxidative stress is the fundamental driver of AMD pathology. It occurs when the production of reactive oxygen species (ROS) exceeds the tissue's antioxidant neutralizing capacity. The retina is particularly rich in polyunsaturated fatty acids (PUFAs), which are prime targets for lipid peroxidation.
- The Role of Antioxidants: The eye relies on exogenous antioxidants—specifically the carotenoids lutein and zeaxanthin, as well as vitamins C and E and zinc—to quench free radicals. Lutein and zeaxanthin accumulate in the macula to form the macular pigment, acting as "internal sunglasses" that filter damaging blue light and stabilize cell membranes.
- Adherence Implication: These nutrients cannot be synthesized by the human body; they must be ingested regularly. Adherence to a diet rich in these compounds is directly correlated with Macular Pigment Optical Density (MPOD). Inconsistent adherence results in fluctuating antioxidant defenses. A "cheat day" in a diabetic diet may cause a transient glucose spike, but in AMD, periods of low antioxidant intake contribute to a cumulative "oxidative debt" that structurally damages the RPE and Bruch's membrane over years, eventually leading to drusen formation and apoptosis.

2.2 Chronic Inflammation and the Complement Cascade
AMD is increasingly recognized as a state of chronic, low-grade inflammation (para-inflammation). The alternative complement pathway, part of the innate immune system, is often dysregulated in AMD patients, leading to attack on the host's own retinal tissues.
- Dietary Modulation: Omega-3 fatty acids (DHA and EPA) serve as precursors to resolvins and protectins, potent anti-inflammatory lipid mediators that dampen this immune response. Conversely, diets high in saturated fats and high-glycemic-index foods trigger systemic inflammation, increasing C-reactive protein (CRP) and complement activation.
- Adherence Implication: The anti-inflammatory effect of omega-3s requires consistent incorporation into cellular membranes, a process that takes weeks to months of steady intake. Sporadic adherence fails to achieve the steady-state membrane concentrations necessary to modulate the complement cascade effectively.
2.3 Vascular Integrity and Endothelial Function
The choroid, the vascular layer supplying the outer retina, has the highest blood flow per unit weight of any tissue in the body. Compromise of the choriocapillaris is an early event in AMD.
- Lifestyle Impact: Smoking introduces potent vasoconstrictors and toxins (e.g., cadmium, reactive aldehydes) that directly damage the choroidal endothelium and reduce choroidal thickness. Sedentary behavior contributes to systemic endothelial dysfunction.
- Adherence Implication: The relationship between smoking and choriocapillaris health is dose-dependent. Every cigarette smoked causes acute vasoconstriction and contributes to cumulative vascular sclerosis. "Cutting down" (partial adherence) provides significantly less benefit than complete cessation (full adherence) due to the high toxicity of tobacco smoke.
3. The Impact of Adherence Levels: Dose-Response Evidence
The scientific literature consistently demonstrates that the protective benefit of lifestyle modification is not a threshold effect but a gradient. The degree of adherence—how closely a patient follows a recommendation—predicts the magnitude of risk reduction.

3.1 Dietary Adherence: The Mediterranean Diet
The Mediterranean diet (MeDi), characterized by high consumption of plant-based foods (vegetables, fruits, legumes, nuts), olive oil as the primary fat, moderate fish intake, and low consumption of red meat and processed foods, provides the most robust evidence base for dietary protection in AMD.

3.1.1 Quantifying Adherence
Research typically quantifies adherence using composite scores (e.g., the Trichopoulou score, ranging from 0 to 9). This methodological rigor allows for the analysis of dose-response relationships. A score of 0-3 represents low adherence, 4-5 moderate, and 6-9 high adherence.
3.1.2 Impact on Disease Progression
A comprehensive systematic review and meta-analysis of prospective cohort studies revealed a statistically significant inverse association between MeDi adherence and AMD progression.
- Hazard Ratios (Prospective Data): Patients with high adherence to the MeDi demonstrated a 23% reduced risk of progressing to advanced AMD (Hazard Ratio = 0.77; 95% CI: 0.67–0.88) compared to those with low adherence.
- Odds Ratios (Case-Control Data): In case-control settings, the protective effect appeared even stronger, with high adherence associated with a 34% reduction in the odds of disease progression (Odds Ratio = 0.66; 95% CI: 0.54–0.81).
- Incident Advanced AMD: The EYE-RISK Consortium, which pooled data from major European cohorts (Rotterdam Study, Alienor Study), found that high adherence to the MeDi was associated with a 41% reduced risk of incident advanced AMD.
3.1.3 Impact on Late-Stage Disease Management
Crucially, the benefits of adherence extend to patients who already have advanced disease. A study examining patients with established advanced AMD found that adherence to the MeDi was significantly associated with a slower rate of progression (enlargement of atrophy or conversion to neovascularization). The rate of slowing was higher in patients who strictly followed the diet compared to those who followed it loosely or not at all (p<0.001). This finding challenges the fatalistic notion that lifestyle changes are futile once the disease has advanced. The data suggests that dietary adherence acts as a metabolic "brake," slowing the degenerative momentum of the disease regardless of stage.
3.2 Nutritional Supplementation: The AREDS Regimen
The Age-Related Eye Disease Studies (AREDS and AREDS2) established a specific formulation of high-dose antioxidants as the standard of care for patients with intermediate AMD or advanced AMD in one eye.
3.2.1 Efficacy and the Adherence Necessity
The AREDS2 formulation (Vitamin C 500mg, Vitamin E 400IU, Lutein 10mg, Zeaxanthin 2mg, Zinc 80mg/25mg, Copper 2mg) reduces the risk of progression to advanced AMD by approximately 25%over five years. Recent post-hoc analyses have also suggested that this formulation may slow the expansion of geographic atrophy, particularly in patients with foveal-sparing lesions, expanding the imperative for adherence to the late dry stage.
However, this benefit is strictly contingent on daily adherence. The pharmacokinetics of these nutrients require consistent dosing to maintain therapeutic tissue levels.
- Real-World Adherence: Adherence rates in clinical practice vary widely, ranging from 38% to 88% depending on the population studied. A hospital-based survey found an adherence rate of 83%, but this likely reflects a motivated, tertiary-care population and may overestimate community adherence.
- Barriers to Supplement Adherence:
- Pill Burden: The regimen often requires multiple pills per day.
- Side Effects: Zinc is known to cause gastrointestinal distress in a subset of patients, leading to discontinuation.
- Cost: These supplements are often not covered by insurance, creating a financial barrier for fixed-income seniors.
- Commercial Misalignment: A significant barrier to effective adherence is the misalignment between commercial products and the evidence-based formula. A study of top-selling eye vitamins found that 30.8% did not adhere to the AREDS2 formula, and many contained sub-therapeutic doses or additional, unproven ingredients. Thus, a patient may be "adherent" to taking a pill daily, but "non-adherent" to the therapeutic regimen due to product selection.

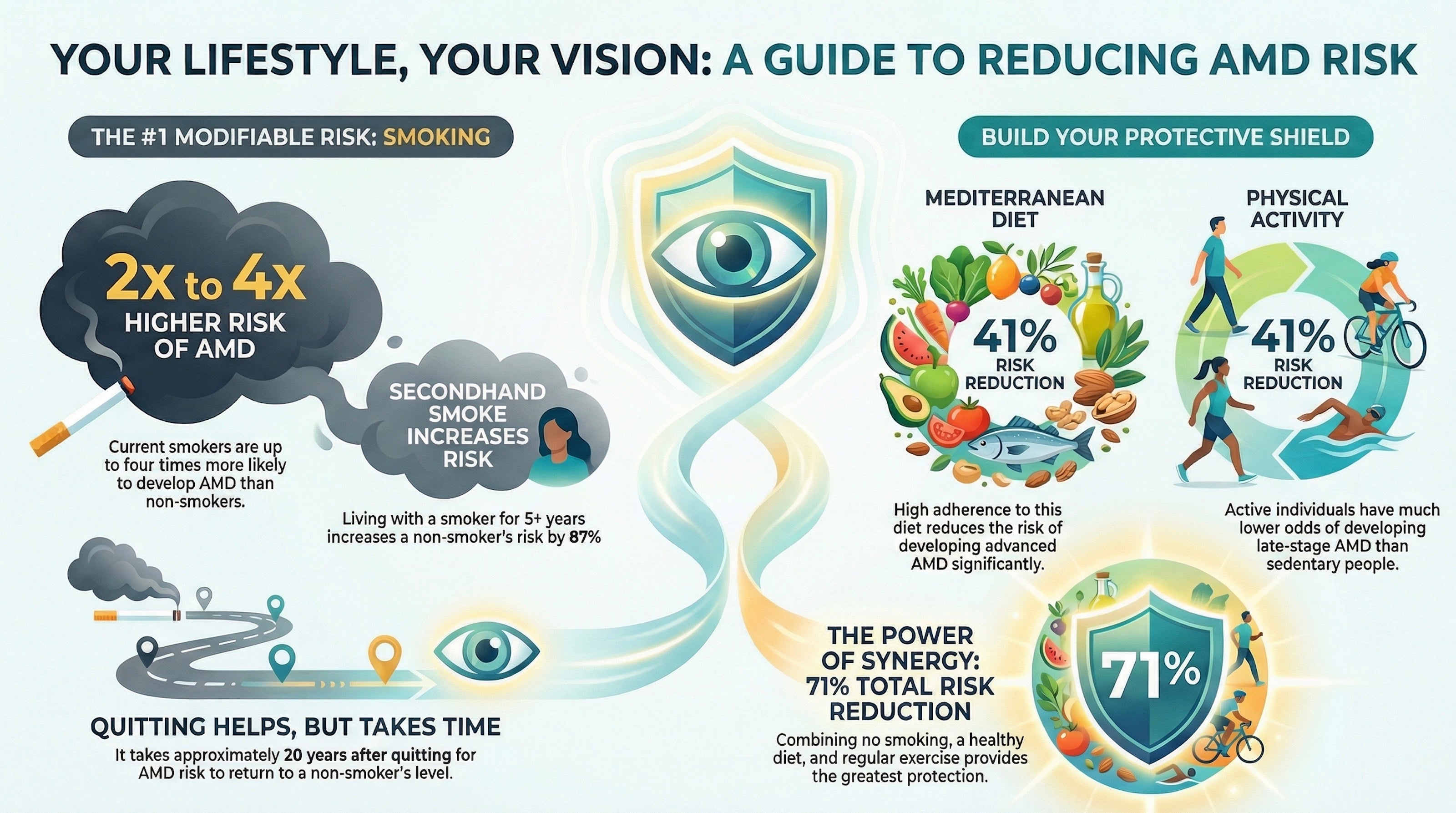
3.3 Smoking Cessation: The Importance of Total Abstinence
Smoking is the strongest modifiable environmental risk factor for AMD.
3.3.1 Dose-Response and Cessation Dynamics
- Increased Risk: Current smokers face a 2- to 4-fold increased risk of developing AMD and a 51.4% higher risk of disease progression compared to never-smokers.
- Intensity of Adherence: The risk is correlated with "pack-years" (cumulative exposure). Women who smoked more than 25 cigarettes per day had a significantly higher risk (OR = 2.4) compared to lighter smokers, emphasizing that even if complete cessation is not achieved, reduction (partial adherence) offers some mitigation, though cessation is the goal.
- Latency of Benefit: Adherence to a smoke-free lifestyle yields benefits that accrue slowly. The Rotterdam Study indicated that the elevated risk of neovascular AMD persists for up to 20 years after cessation. The Nurses' Health Study found a 2-fold increased risk even 15 years after quitting for heavy smokers. This data underscores the critical importance of earlyadherence to cessation; waiting until diagnosis to quit may leave the patient with a "legacy effect" of risk that takes decades to normalize.
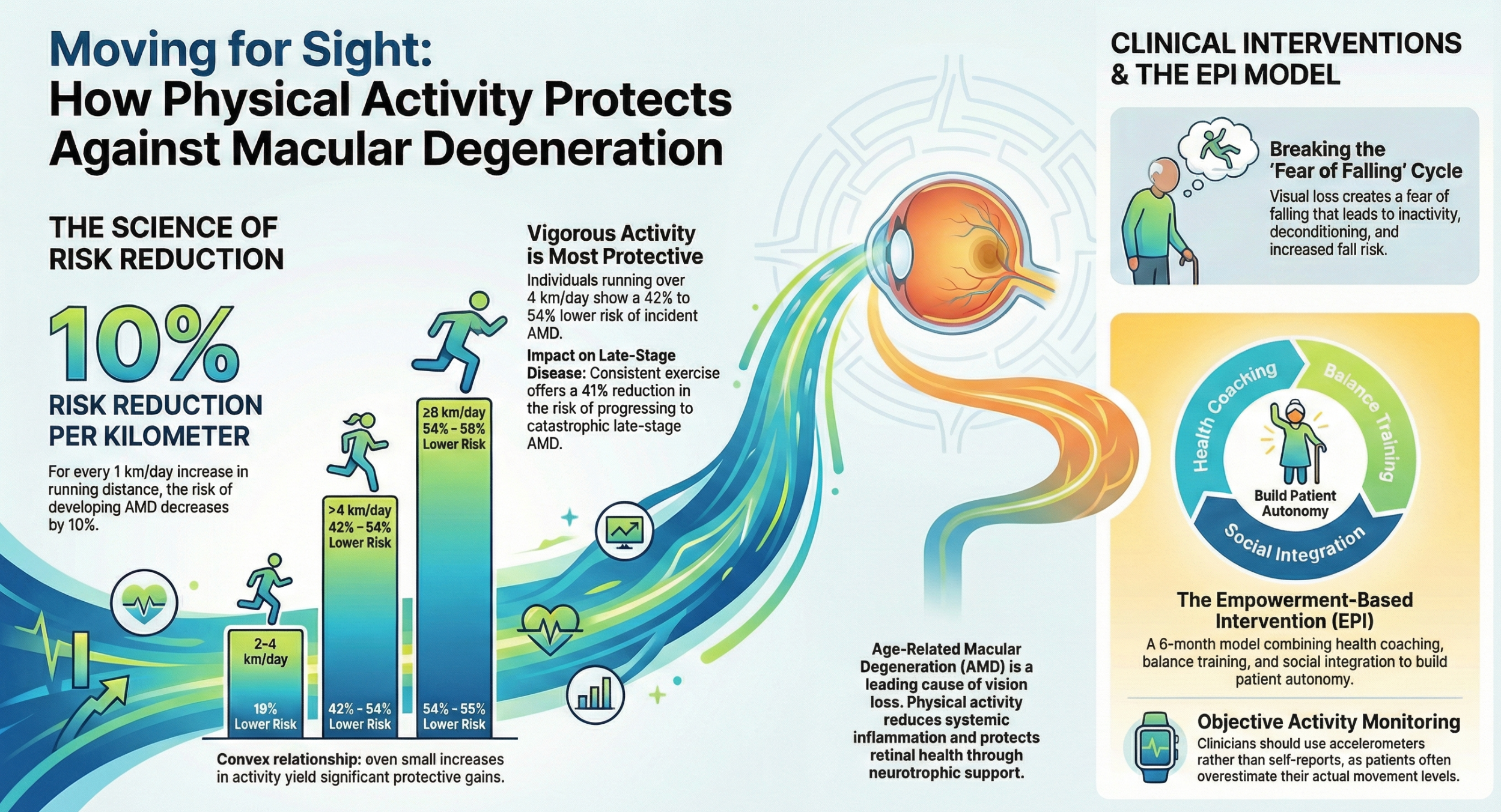
3.4 Physical Activity
Physical activity (PA) influences AMD risk through systemic vascular health, inflammation reduction, and oxidative stress modulation.
3.4.1 Intensity and Consistency
- Risk Reduction: High levels of physical activity have been associated with a 42% to 54% reduction in AMD risk. Conversely, sedentary behavior is a risk factor; low-to-moderate activity levels were associated with a 19% higher risk of early AMD compared to high activity levels (HR = 1.19).
- Adherence Metrics: The definition of "adherence" in PA studies varies, but generally, adherence to guidelines (e.g., 150 minutes of moderate activity per week) correlates with protection. Notably, the protective effect appears strongest for preventing incidence of early AMD, while the data on preventing progression to late AMD is more mixed. This suggests that PA adherence may be most critical in the preclinical or very early stages of the disease.
3.5 Combined Lifestyle Adherence: The Synergistic Effect
The most compelling evidence for adherence comes from studies evaluating the cumulative impact of multiple healthy behaviors.
- Composite Healthy Lifestyle Scores: Researchers have developed "Healthy Lifestyle Scores" (HLS) aggregating diet, smoking status, and physical activity.
- Magnitude of Effect: In the Carotenoids in Age-Related Eye Disease Study (CAREDS), women with high HLS (adherence to 3 healthy behaviors) had 71% lower odds of AMD compared to those with low scores.
- The Genetic Interaction (Synergy): Perhaps the most critical finding for patient counseling is the interaction between genetics and lifestyle. Individuals with high-risk genotypes (e.g., CFHY402H homozygotes) have a significantly elevated baseline risk. However, strict adherence to a healthy lifestyle can dampen this genetic predisposition.
- Data Point: A study showed that in high-genetic-risk individuals, adherence to a healthy lifestyle reduced the odds of AMD from 3.21 (in the low-adherence group) to 0.98 (in the high-adherence group).Essentially, adherence neutralized the excess genetic risk.
- Synergy Index: The combination of high genetic risk and low lifestyle adherence produces a risk greater than the sum of the individual risks (Synergy Index = 1.34). This implies that adherence is more important for genetically susceptible individuals than for the general population.

4. Barriers to Adherence: The "Adherence Gap"
Despite the overwhelming evidence supporting lifestyle modification, real-world adherence remains suboptimal. Understanding the specific barriers preventing patients from adhering is essential for designing effective interventions. The "COM-B" model (Capability, Opportunity, Motivation - Behavior) provides a useful framework for analyzing these barriers.
4.1 Psychological Barriers (Motivation and Capability)
- Fatalism and Depression: A diagnosis of AMD often triggers a grief reaction related to the loss of vision. Many patients adopt a fatalistic worldview ("I'm going blind anyway"), which obliterates the motivation to change diet or exercise habits. Depression, prevalent in AMD populations, is itself a barrier to behavioral activation.
- Knowledge Deficits: There is a profound lack of "health literacy" regarding the eye-body connection. Patients frequently compartmentalize their health; they may understand that exercise helps the heart but fail to see its relevance to the retina. Qualitative interviews reveal confusion ("Is this for the eyes or for the body?") and skepticism about the efficacy of non-pharmacological interventions.
- Invisible Efficacy: Prevention is invisible. Adherence to a diet does not result in an immediate improvement in vision; it merely (hopefully) prevents deterioration. This lack of positive reinforcement makes sustaining motivation difficult.

4.2 Physical and Functional Barriers (Capability)
- Visual Impairment: The functional limitations of AMD directly impede adherence to lifestyle recommendations.
- Diet: Reading nutrition labels, identifying fresh produce, and cooking safely are challenging with central scotomas.
- Exercise: Fear of falling is high among visually impaired seniors, leading to self-restriction of mobility and physical activity.
- Medication Management: Difficulty reading pill bottles or distinguishing between supplements contributes to unintentional non-adherence.
4.3 Social and Environmental Barriers (Opportunity)
- Social Isolation: Vision loss restricts driving and independent travel, leading to social withdrawal. Social support is a primary enabler of adherence; eating is often a social activity, and isolation often leads to reliance on convenient, processed foods rather than home-cooked, nutrient-dense meals.
- Food Environment and Cost: The components of a Mediterranean diet (fresh fish, nuts, produce) are often more expensive than processed alternatives. For elderly patients on fixed incomes, this cost barrier is significant. Similarly, AREDS2 supplements represent an out-of-pocket expense that can be prohibitive.
4.4 Systemic and Provider Barriers
- Lack of Physician Recommendation: While ophthalmologists universally recommend smoking cessation, recommendations for diet and weight management are less consistent (42% and 37% respectively in one survey).
- Time Constraints: In high-volume retinal clinics, the focus is often on imaging and injections. Detailed lifestyle counseling is frequently deprioritized due to time pressure and a lack of reimbursement for such services.
5. Methods to Improve Adherence: Evidence-Based Interventions
Addressing the "adherence gap" requires moving beyond passive advice-giving to active, structured behavioral interventions. The user query specifically asks about the role of coaching and other methods to improve adherence. The literature identifies several promising modalities.

5.1 Health Coaching and Personalized Risk Profiling
Health coaching is a patient-centered approach where a provider (coach) facilitates the patient in setting goals, identifying barriers, and monitoring progress. It differs from education by focusing on empowerment and accountability.
5.1.1 The AMD-Life Study
The "AMD-Life" study represents the most significant effort to rigorously test the impact of coaching on lifestyle adherence in AMD patients.
- Study Design: This randomized clinical trial compared three arms:
- Standard Care: Standard lifestyle recommendations and free supplements.
- Risk Profiling: Standard care plus a personalized risk assessment based on genetics (phenotype) and environmental factors.
- Coaching: Risk profiling plus professional health coaching.
- Findings: Preliminary results indicated a hierarchy of efficacy. Patients who received personalized risk assessments improved their lifestyle scores significantly more than the standard care group (mean difference 1.70, p<0.05). However, the group that received coaching showed the greatest improvement (mean difference 3.0, p<0.001).
- Mechanism: The study suggests a two-stage mechanism for adherence. First, Personalized Risk Profilingconverts abstract risks into concrete, personal threats, increasing "reflective motivation." Second, Coachingprovides the "scaffolding" necessary to translate that motivation into sustained action, using techniques like goal setting and feedback.

5.1.2 General Efficacy of Coaching
In broader chronic disease management (diabetes, cardiovascular disease), health coaching has consistently demonstrated improvements in adherence and clinical outcomes. It has been shown to be a cost-effective intervention, particularly for patients with multiple comorbidities, a profile that matches many AMD patients.
5.2 Motivational Interviewing (MI)
Motivational Interviewing is a counseling method designed to resolve ambivalence about change. It is particularly useful for patients who are "stuck" or resistant.
- Evidence in Ophthalmology: While direct studies in AMD are limited, evidence from glaucoma (another chronic, progressive eye disease) is compelling. A study of African descent patients with poor glaucoma medication adherence found that an MI intervention significantly improved adherence from 56% to 68%(p=0.03), whereas the control group showed no improvement.
- Nuance: Not all MI interventions are superior to simple reminders. One study found that for patients with highbaseline adherence, automated reminders were more cost-effective than MI. This suggests a stratified approach: use automated tools for the majority, and reserve resource-intensive MI/coaching for those with demonstrated non-adherence.
5.3 Digital Health Interventions
Technology offers scalable solutions to the adherence problem, though accessibility for the visually impaired remains a design challenge.
5.3.1 Smartphone Apps and Nutrient Tracking
- Feasibility: A feasibility study demonstrated that AMD patients (median age 57) could successfully use a smartphone app to record dietary intake. The app's analysis of key nutrients (lutein, zeaxanthin, omega-3s) showed high agreement with dietitian-analyzed paper diaries, but with significantly lower burden.
- Mechanism: These apps provide Self-Monitoring, a core Behavior Change Technique (BCT). By seeing their daily nutrient "score," patients receive immediate feedback, reinforcing the behavior.
- Medication Adherence: In broader cardiovascular studies, app-based reminders have improved medication adherence by over 14 percentage points.
- Home Monitoring: Devices like the "ForeseeHome" or apps like "Alleye" allow patients to monitor their vision at home. While primarily diagnostic, these tools keep the patient "engaged" with their condition daily. High engagement in monitoring often spills over into better adherence to other regimens. Economic models show these interventions are cost-effective ($35,663/QALY) for high-risk patients.

5.4 Peer Support and Group Interventions
Social support addresses the isolation barrier and provides "vicarious experience"—seeing peers succeed makes the patient believe they can too.
- The MINGLE Program: This intervention ("Movement, Interaction and Nutrition for Greater Lifestyles in the Elderly") utilized group sessions to promote adherence. Qualitative analysis identified "socializing" as a primary enabler. Patients were motivated to attend not just for the health information, but for the connection with others facing similar challenges. The group setting allowed for the sharing of practical "hacks" (e.g., how to cook with low vision), effectively increasing the "capability" of participants.
- Efficacy: Peer-facilitated interventions in other chronic diseases have shown lower attrition rates and higher adherence to medication and exercise compared to solitary interventions.
Table 1: Comparative Efficacy of Adherence Interventions
|
Intervention Type |
Mechanism of Action |
Evidence Base |
Key Findings/Impact |
|
Health Coaching |
Facilitation, accountability, goal setting |
AMD-Life Study |
Highest impact: Mean lifestyle score improvement of 3.0 vs standard care. |
|
Personalized Risk Profiling |
Increases risk perception (Motivation) |
AMD-Life Study |
Significant improvement over standard care (1.70), but less than coaching. |
|
Motivational Interviewing |
Resolves ambivalence |
Glaucoma Studies |
Improved adherence from 56% to 68% in non-adherent populations. |
|
Digital Apps |
Self-monitoring, reminders |
Nutritional Studies |
Feasible for nutrient tracking; improves medication adherence by ~14%. |
|
Peer Support |
Social scaffolding, vicarious learning |
MINGLE Program |
High engagement; reduces isolation barriers; improves retention. |
6. Economic Implications: The Value of Adherence
The imperative for adherence is not solely clinical; it is also economic. The cost of treating advanced AMD is staggering, involving frequent specialist visits, expensive biologic drugs (anti-VEGF), and the extensive costs of low-vision rehabilitation and lost productivity.
6.1 Cost-Effectiveness of Prevention
- Supplementation: Economic modeling has demonstrated that AREDS supplementation is a dominant cost-effective intervention for patients with intermediate to advanced AMD. By preventing the transition to neovascular disease (and the associated anti-VEGF costs), supplementation yields a cost-effectiveness ratio of $21,387 per Quality-Adjusted Life Year (QALY) gained, far below the typical willingness-to-pay threshold of $50,000-$100,000/QALY.For Category 4 patients, it is often cost-saving.
- Lifestyle Interventions: A specific analysis of preventing advanced AMD via a combined supplement (RQC - Resveratrol, Quercetin, Curcumin) estimated that preventing 68% of new cases could yield $1.4 to $3.9 billion in annual direct treatment cost savings in the US alone. Additionally, preventing the progression to legal blindness (20/200 or worse) would save an additional $272 million annually in incremental burden costs.
- Screening and Early Lifestyle Intervention: Decision-analytic Markov models applied to populations in China suggest that combined screening for AMD and lifestyle intervention is highly cost-effective in both rural and urban settings, potentially averting hundreds of years of blindness per 100,000 people screened.

6.2 The Cost of Non-Adherence
Conversely, non-adherence carries a heavy price tag. The macroeconomic costs of visual disability in Europe are estimated at up to €100 billion. Even a modest reduction in adherence that accelerates the onset of advanced disease by 1-2 years shifts patients into high-cost care tiers earlier, compounding the economic burden. Furthermore, commercial non-compliance (patients buying the "wrong" supplements) represents a "wasted" expenditure of millions of dollars annually by consumers who receive no therapeutic benefit.

7. Discussion: Synthesizing the Adherence Paradigm
7.1 The "Adherence Gap" as a Therapeutic Target
The data presented reveals that lifestyle factors are potent modifiers of AMD progression, potentially neutralizing genetic risk. However, the "drug" of lifestyle is only effective if the "dose" (adherence) is sufficient. The current clinical landscape is characterized by an "adherence gap"—the chasm between the 50-70% risk reduction seen in high-adherence cohorts and the 40-60% adherence rates seen in practice. Closing this gap is arguably the most accessible "new treatment" available for AMD.
7.2 The Synergistic Role of Genetics
The interaction between genetics and lifestyle (the Synergy Index) is a critical insight for patient counseling. Patients with high genetic risk are often the most fatalistic, yet the data proves they are the ones who stand to gain the most from strict adherence. This paradox suggests that genetic testing should not be viewed merely as a prognostic tool, but as a motivational tool. As demonstrated in the AMD-Life study, showing a patient their specific genetic risk—and crucially, how lifestyle can mitigate it—can be the catalyst for "reflective motivation" that drives adherence.
7.3 Integration into Clinical Practice
For ophthalmologists and optometrists, the implication is that "advice giving" is an insufficient intervention. The standard of care must evolve to include structured adherence support:
- Referral Pathways: Establishing referral networks with health coaches, dietitians, and smoking cessation counselors.
- Prescription of Digital Tools: Actively prescribing validated apps for diet tracking or vision monitoring to maintain patient engagement between visits.
- Risk Communication: utilizing personalized risk calculators to visualize the benefit of adherence for the patient.
7.4 Future Research Directions
Future research must prioritize:
- Long-term Durability: Determining if the effects of coaching persist after the intervention ends.
- Standardization: developing standardized metrics for "lifestyle adherence" to allow for better meta-analysis.
- Reimbursement: Developing economic models to support the reimbursement of lifestyle coaching in ophthalmology, currently a major systemic barrier.

8. Conclusion
The scientific evidence is unequivocal: adherence to a healthy lifestyle—comprising a Mediterranean diet, smoking cessation, physical activity, and appropriate supplementation—is a powerful therapeutic tool in the management of Age-Related Macular Degeneration. It offers the potential to reduce the risk of progression to vision-threatening disease by up to 70%, particularly in genetically susceptible individuals.

However, the passive dissemination of recommendations has failed to achieve the necessary levels of adherence required to realize these benefits at a population level. The future of AMD management lies in behavioral precision medicine: utilizing genetic risk profiling to target interventions, employing health coaches to facilitate change, and leveraging digital tools to maintain engagement. Adherence is not merely a patient responsibility but a systemic challenge that requires a fundamental re-engineering of ophthalmic care delivery to support the sustained behavioral changes necessary to preserve vision.
Watch the blog summary video on Youtube by clicking here.....
or watch the video on Facebook by clicking here.....
References
- Systematic review on lifestyle behaviors and AMD risk.https://pubmed.ncbi.nlm.nih.gov/41076031/
- Meta-analysis of Mediterranean diet and AMD progression.https://pubmed.ncbi.nlm.nih.gov/40292456/
- Potential of lifestyle intervention to reduce disease progression.https://scholarlypublications.universiteitleiden.nl/access/item%3A3643509/view
- Adherence to Med Diet delaying AMD progression.https://pubmed.ncbi.nlm.nih.gov/37369498/
- Impact of Med Diet on advanced AMD progression rates.https://iv.iiarjournals.org/content/37/4/1809
- Mediterranean diet and ocular diseases review. https://www.mdpi.com/2072-6643/16/18/3169
- AREDS/AREDS2 major findings. https://www.nei.nih.gov/eye-health-information/clinical-trials/age-related-eye-disease-studies-aredsareds2/about-areds-and-areds2
- Adherence to AREDS recommendations in tertiary care.https://pubmed.ncbi.nlm.nih.gov/40374301/
- Variable rates of adherence to AREDS guidelines. https://www.e-retina.or.kr/journal/view.html?doi=10.21561/jor.2022.7.2.121
- AREDS2 supplements for late dry AMD.https://www.macularsociety.org/about/media/news/2024/july/areds2-supplements-slow-sight-loss-in-late-stage-dry-amd/
- Barriers to lifestyle modification in AMD (MINGLE).https://pmc.ncbi.nlm.nih.gov/articles/PMC10958751/
- Psychological and physical barriers to adherence.https://bmjopen.bmj.com/content/12/11/e064892
- Enablers and barriers to MINGLE participation.https://www.researchgate.net/publication/375400609_Understanding_barriers_and_enablers_to_participation_in_a_proposed_online_lifestyle_intervention_for_older_adults_with_age-related_macular_degeneration_to_guide_programme_implementation
- AMD-Life study preliminary findings on coaching. https://iovs.arvojournals.org/article.aspx?articleid=2789866
- AMD-Life study design: Coaching arm. https://pmc.ncbi.nlm.nih.gov/articles/PMC9920008/
- Feasibility of personal risk profiling and coaching.https://onderzoekmetmensen.nl/en/node/54691/pdf
- Motivational interviewing vs reminder calls.https://pmc.ncbi.nlm.nih.gov/articles/PMC5560586/
- Motivational interviewing in glaucoma adherence. https://iovs.arvojournals.org/article.aspx?articleid=2335022
- Motivational interviewing mechanisms. https://pharmaceutical-journal.com/article/ld/using-motivational-interviewing-to-improve-medicines-adherence
- Dose-response of Mediterranean diet score. https://www.mdpi.com/2072-6643/17/6/1037
- EYE-RISK Consortium findings on diet and advanced AMD.https://www.researchgate.net/publication/335235224_Mediterranean_Diet_and_Incidence_of_Advanced_Age-Related_Macular_Degeneration_The_EYE-RISK_Consortium
- European Eye Study: Med Diet Score and AMD.https://www.aao.org/eyenet/article/mediterranean-diet-score-amd-european-eye-study
- Smoking and diet impact on progression.https://pmc.ncbi.nlm.nih.gov/articles/PMC10347925/
- Smoking cessation and long-term risk. https://pmc.ncbi.nlm.nih.gov/articles/PMC3866712/
- Health Canada: Smoking and AMD risk. https://www.canada.ca/en/health-canada/services/health-concerns/tobacco/legislation/tobacco-product-labelling/smoking-related-macular-degeneration.html
- Potential of lifestyle intervention and cost. https://www.mdpi.com/2072-6643/15/3/602
- Smoking as leading manageable risk factor. https://www.vrcny.com/blog/exploring-the-link-between-smoking-and-amd-facts-and-risks
- Ophthalmologist recommendations for lifestyle.https://pmc.ncbi.nlm.nih.gov/articles/PMC8815001/
- Physical activity and 15-year incidence. https://iovs.arvojournals.org/article.aspx?articleid=2212634
- Running distance and AMD risk reduction.https://pmc.ncbi.nlm.nih.gov/articles/PMC4090325/
- High levels of PA protective for early AMD. https://pubmed.ncbi.nlm.nih.gov/34695401/
- Meta-analysis of physical activity and AMD. https://www.aao.org/eyenet/article/physical-activity-protects-against-amd
- Combined healthy lifestyle score and genotype. https://iovs.arvojournals.org/article.aspx?articleid=2146955
- CAREDS: Healthy lifestyle score and AMD odds.https://pmc.ncbi.nlm.nih.gov/articles/PMC3075357/
- AMD-Life study details. https://clinicaltrials.gov/study/NCT05667441
- Interaction of healthy lifestyle and genotype.https://pmc.ncbi.nlm.nih.gov/articles/PMC4714866/
- Composite LE8 score and AMD incidence. https://iovs.arvojournals.org/article.aspx?articleid=2802901
- Diagnostic performance of mobile apps (Alleye).https://pmc.ncbi.nlm.nih.gov/articles/PMC9999269/
- Cost-effectiveness of health coaching. https://pmc.ncbi.nlm.nih.gov/articles/PMC5312514/
- Costs of health coaching intervention. https://www.ajmc.com/view/costs-for-a-health-coaching-intervention-for-chronic-care-management
- Peer-facilitated interventions and adherence.https://pmc.ncbi.nlm.nih.gov/articles/PMC5695224/
- Cost-effectiveness of vitamin therapy (AREDS). https://pubmed.ncbi.nlm.nih.gov/17320962/
- Economic impact of RQC prevention. https://iovs.arvojournals.org/article.aspx?articleid=2805041
- Cost-effectiveness of home monitoring. https://pmc.ncbi.nlm.nih.gov/articles/PMC5470421/
- CRN Foundation economic report on lutein. https://www.crnusa.org/newsroom/crn-foundations-economic-report-outlines-value-lutein-and-zeaxanthin-reducing-medical
- Dietary intervention cost-effectiveness. https://www.mdpi.com/2072-6643/16/23/4124
- Text message reminders and adherence.https://pmc.ncbi.nlm.nih.gov/articles/PMC5561384/
- Feasibility of mobile app for nutrient intake.https://pmc.ncbi.nlm.nih.gov/articles/PMC5270627/
- COM-B model and nutrition intervention. https://bmjopen.bmj.com/content/12/11/e064892
- Cost-effectiveness of telescreening in China.https://pmc.ncbi.nlm.nih.gov/articles/PMC8958534/
- Macular pigment as biomarker. https://www.crnusa.org/sites/default/files/HCCS/06-CRN-Supplements-to-Savings-2022-MPOD-LuteinZeaxanthin.pdf
- Compliance of commercial supplements.https://pmc.ncbi.nlm.nih.gov/articles/PMC10257890/
- Financial burden and AREDS abstinence. https://pubmed.ncbi.nlm.nih.gov/20602323/
- Economic burden of AMD in Europe. https://pmc.ncbi.nlm.nih.gov/articles/PMC9920008/
- Mobile phone app vs food diary. https://pmc.ncbi.nlm.nih.gov/articles/PMC5270627/
- Systematic review of lifestyle factors (2025).https://pmc.ncbi.nlm.nih.gov/articles/PMC11946629/
- MINGLE program barriers and enablers.https://pmc.ncbi.nlm.nih.gov/articles/PMC10958751/
- Systematic review AMD progression odds. https://pubmed.ncbi.nlm.nih.gov/40292456/
- Economic savings of AMD prevention. https://iovs.arvojournals.org/article.aspx?articleid=2805041
{kind=link}
Leave a comment
This site is protected by hCaptcha and the hCaptcha Privacy Policy and Terms of Service apply.