Modifiable Determinants of Retinal Health: An Exhaustive Analysis of Lifestyle Interventions in the Management of Age-Related Macular Degeneration
1. Introduction: The Evolving Landscape of Ophthalmic Epidemiology
Age-Related Macular Degeneration (AMD) stands as the preeminent cause of irreversible blindness in the developed world, a distinction that carries with it profound public health implications as global populations undergo a demographic shift toward advanced age. Historically, the prevailing clinical dogma viewed AMD largely as an inevitable consequence of senescence—a "wear and tear" phenomenon dictated by the immutable ticking of the biological clock and the fixed hand of genetic inheritance. For decades, the therapeutic landscape was characterized by a sense of nihilism, offering patients little beyond visual aids and grim prognoses. However, the last quarter-century has witnessed a paradigm shift, transitioning from a model of genetic determinism to one of epigenetic modification, where environmental inputs and lifestyle choices play a decisive role in the trajectory of retinal health.

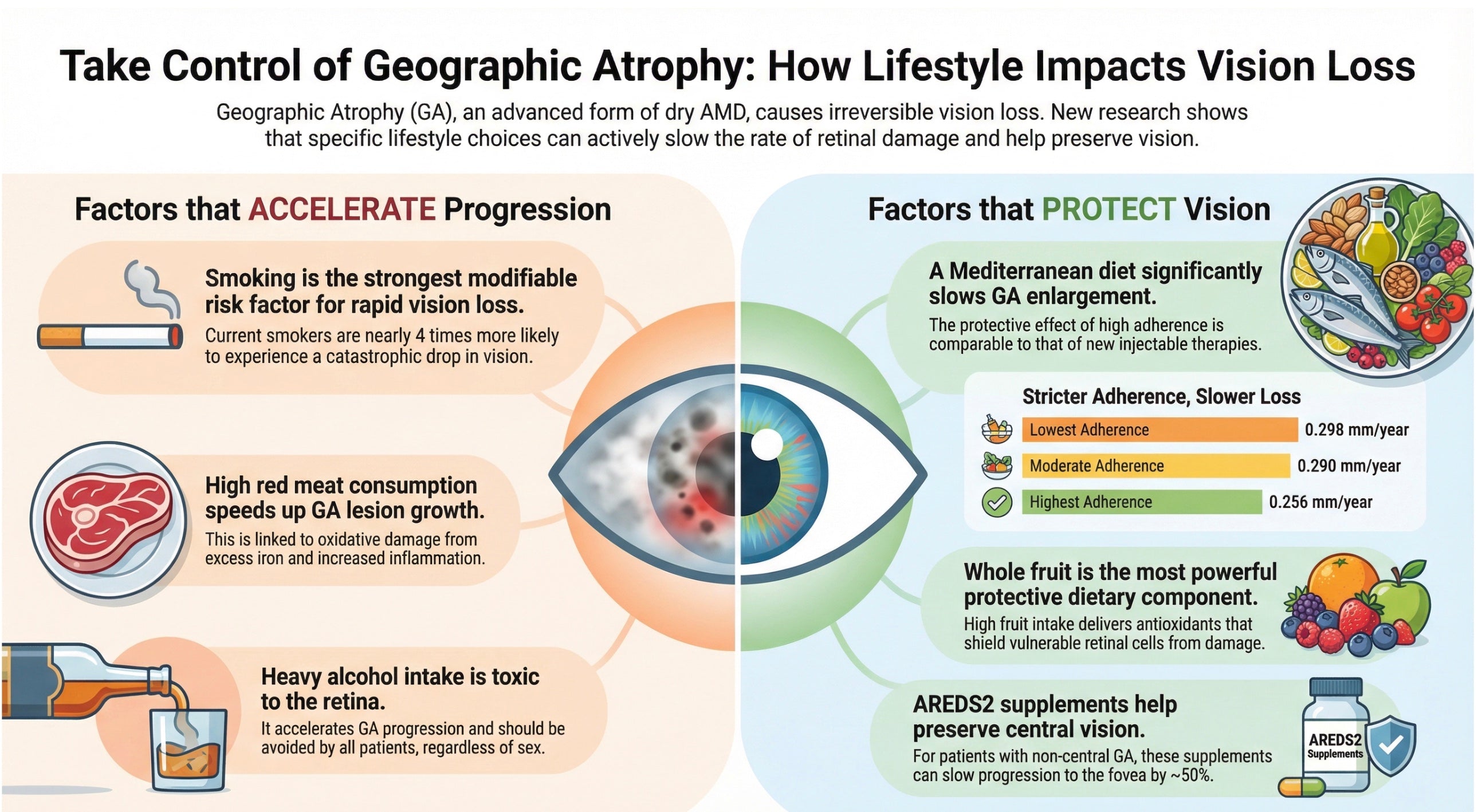
The urgency of this shift is underscored by the staggering epidemiological projections. Current estimates suggest that the global prevalence of AMD will surge to nearly 300 million individuals by the year 2040.1 This looming crisis is not merely a function of longer life expectancies but also reflects the cumulative impact of modern lifestyle factors that accelerate retinal aging. The disease manifests in two primary late-stage phenotypes: neovascular (wet) AMD, characterized by the aberrant growth of choroidal blood vessels and subsequent leakage, and geographic atrophy (dry AMD), characterized by the progressive, confluent death of the retinal pigment epithelium (RPE) and photoreceptors. While the advent of anti-vascular endothelial growth factor (anti-VEGF) therapies has revolutionized the management of wet AMD, these treatments are reactive, burdensome, and do not address the underlying degenerative processes. Furthermore, until very recently, no effective treatments existed for geographic atrophy, making primary prevention the only viable strategy for preserving vision in millions of at-risk individuals.2

Recent large-scale epidemiological investigations have fundamentally altered our understanding of AMD risk. It is now established that while genetic variants—most notably in the Complement Factor H (CFH) and ARMS2 genes—confer susceptibility, they do not seal a patient’s fate. Instead, lifestyle factors act as potent effect modifiers. The evidence suggests that modifiable behaviors, specifically dietary patterns, physical activity, and smoking habits, interact dynamically with a patient's genetic substrate to determine whether susceptibility translates into blindness.3 This report provides a comprehensive, evidence-based synthesis of the role of these lifestyle factors. By dissecting the statistical magnitude of risk reduction, exploring the molecular mechanisms of protection, and analyzing the synergies between behaviors, we aim to provide a definitive resource for understanding how lifestyle modification can serve as a primary therapeutic modality in the management of AMD.

2. The Pathophysiological Basis of Lifestyle Intervention
To understand how macroscopic behaviors like diet and exercise influence the microscopic health of the retina, one must first appreciate the unique metabolic vulnerability of the macula. The retina is the most metabolically active tissue in the human body per unit weight, consuming oxygen at a rate that exceeds even that of the brain. This hyper-metabolism is necessary to support the phototransduction cascade—the conversion of light energy into electrical signals—but it comes at a steep physiological cost: the continuous generation of Reactive Oxygen Species (ROS).4
2.1 Oxidative Stress and the RPE
The Retinal Pigment Epithelium (RPE) performs a critical housekeeping function, phagocytosing the shed outer segments of photoreceptors daily. This process is inherently oxidative. In a healthy eye, an endogenous antioxidant defense system, regulated by pathways such as Nrf2, neutralizes these free radicals. However, lifestyle factors like smoking introduce an overwhelming exogenous load of oxidants, while poor diet deprives the RPE of the exogenous antioxidants (e.g., lutein, zeaxanthin, vitamin C) required to replenish its defenses.5 When the oxidative burden exceeds the antioxidant capacity, lipids within the photoreceptor membranes undergo peroxidation. These oxidized lipids and proteins accumulate as lipofuscin within the RPE, eventually aggregating to form drusen—the hallmark deposits of AMD.
2.2 Chronic Inflammation and the Inflammasome
Oxidative stress is inextricably linked to inflammation. The accumulation of cellular debris and oxidized byproducts triggers the immune system, specifically the complement cascade. In AMD, this inflammatory response becomes chronic and maladaptive. A key molecular player in this process is the NLRP3 inflammasome, an intracellular protein complex that detects "danger signals" such as amyloid-beta or oxidized LDL (common components of drusen). Upon activation, the inflammasome triggers the release of pro-inflammatory cytokines like Interleukin-1β (IL-1β) and Interleukin-18 (IL-18), which drive RPE cell death via pyroptosis.5
Lifestyle interventions exert their protective effects by modulating this inflammatory axis. For instance, omega-3 fatty acids found in the Mediterranean diet serve as precursors to specialized pro-resolving mediators (resolvins) that actively dampen inflammasome activation. Conversely, physical activity stimulates the release of myokines from skeletal muscle that have systemic anti-inflammatory effects.
2.3 Vascular Integrity and Perfusion
The choroid, the vascular layer supplying the outer retina, has the highest blood flow rate of any vascular bed. This torrential flow is required not just for oxygen delivery, but to act as a heat sink, dissipating the thermal energy generated by focused light. Aging and cardiovascular disease (hypertension, atherosclerosis) lead to choroidal thinning and reduced choriocapillaris density. Physical activity plays a crucial role here by enhancing endothelial function and maintaining pulsatile ocular blood flow, thereby ensuring efficient waste clearance across Bruch’s membrane. The "vascular hypothesis" of AMD suggests that ischemia—often driven by smoking-induced vasoconstriction or sedentary-induced endothelial dysfunction—is a primary driver of drusen formation and neovascular conversion.6

3. Tobacco Use: The Primary Environmental Insult
Of all the modifiable risk factors identified in ophthalmic epidemiology, cigarette smoking stands out as the most potent, consistent, and devastating environmental insult to the retina. The statistical association is robust, reproducible across diverse ethnic populations, and exhibits a clear dose-response relationship that implicates tobacco toxicity directly in the pathogenesis of blindness.
3.1 Quantifying the Risk: A Statistical Imperative
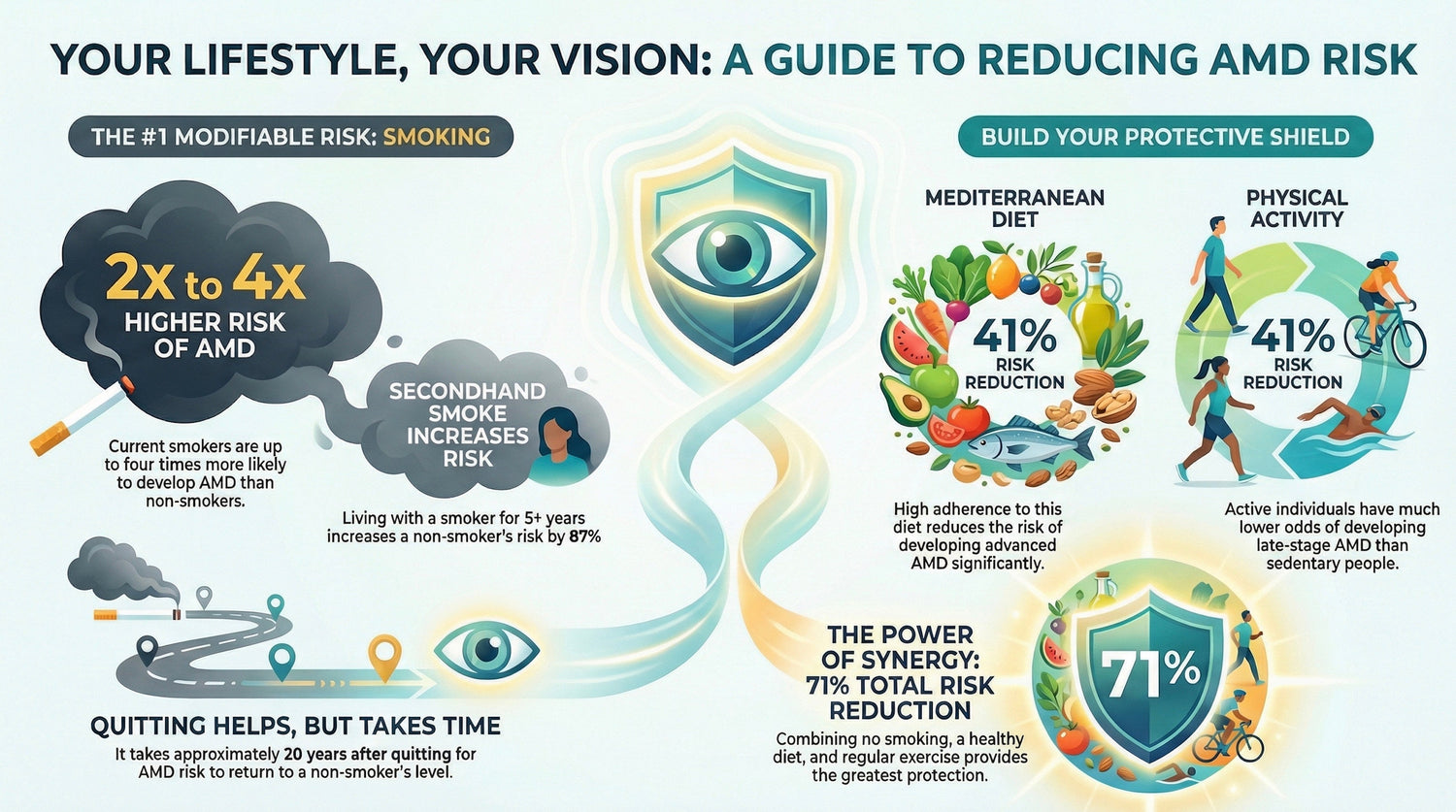
The magnitude of risk conferred by smoking is profound. A meta-analysis comprising six prospective cohort studies, five case-control studies, and five cross-sectional studies established that current smokers face an Odds Ratio (OR) of developing AMD ranging from 2.39 to 4.22 compared to those who have never smoked.8 This places smoking as the second most consistent risk factor for AMD, surpassed only by age itself.

The risk is not uniform across all smokers; it is heavily dependent on the intensity and duration of the habit, quantified in "pack-years." Research utilizing detailed questionnaires has demonstrated a stark linear progression in risk:
- Heavy Smokers (>40 pack-years): Individuals with a history of more than 40 pack-years have an odds ratio of 3.43 (95% CI: 1.28–9.20) for developing geographic atrophy and 2.49 (95% CI: 1.06–5.82) for neovascular AMD.9
- Moderate Smokers (20-40 pack-years): The risk remains elevated but lower, with odds ratios hovering around 1.5 to 1.6 for both subtypes.10
- Passive Exposure: The danger extends beyond the smoker. Non-smokers who have lived with a smoker for five years or more exhibit an odds ratio of 1.87 (95% CI: 1.03–3.40) for developing AMD.9 This finding is critical for public health messaging, highlighting that "secondhand smoke" is a significant ocular hazard.
In terms of global disease burden, the impact is staggering. Spatiotemporal analyses of the Global Burden of Disease data indicate that smoking-attributable AMD resulted in nearly 60,000 Years Lived with Disability (YLDs) globally in 2021 alone.11 In China, a country with high smoking prevalence, the number of YLDs attributable to smoking-induced AMD rose by 184% between 1990 and 2021, illustrating how the aging of the population amplifies the consequences of tobacco use.12
3.2 Mechanisms of Tobacco-Induced Retinal Toxicity
Tobacco smoke is a complex aerosol containing over 4,000 chemical compounds, many of which are directly toxic to ocular tissues.
- Oxidative Depletion: Cigarette smoke is a rich source of pro-oxidants. Systemic absorption of these compounds depletes the body’s reserves of antioxidants, including plasma vitamin C and macular carotenoids. Smokers consistently demonstrate lower Macular Pigment Optical Density (MPOD) than non-smokers, leaving their photoreceptors vulnerable to blue light damage.6
- Complement Dysregulation: Smoking has been shown to alter the expression of complement regulatory proteins. In individuals who already harbor high-risk alleles in CFH—essentially having a "fragile" complement system—smoking acts as a catastrophic "second hit." It lowers the threshold for alternative pathway activation, leading to unchecked inflammation and drusen biogenesis.13
- Vascular Compromise: Nicotine induces acute vasoconstriction and chronic endothelial dysfunction. Since the choriocapillaris requires high flow to sustain the RPE, the chronic ischemia induced by smoking promotes hypoxia. The RPE responds to hypoxia by upregulating Vascular Endothelial Growth Factor (VEGF), thereby directly promoting the transition to the neovascular (wet) form of the disease.14
- Cadmium Accumulation: Tobacco accumulates cadmium from the soil. Cadmium is a heavy metal that competes with zinc, an essential mineral for retinal metalloenzymes. The accumulation of cadmium in the RPE/choroid complex of smokers has been posited as a mechanism for RPE toxicity.
3.3 Cessation: The Timeline of Recovery
A critical question for clinicians and patients is the reversibility of this risk. The data suggests that while the damage is cumulative, cessation offers significant benefits, though the timeline to full risk normalization is protracted.
- Immediate Benefits: Current smokers develop neovascular AMD on average 5.5 years earlier than never-smokers.15 This implies that cessation can significantly delay the onset of vision loss, preserving quality of life during the patient's most active senior years.
- Long-Term Normalization: The risk profile of former smokers improves slowly. It takes approximately 20 years of cessation for the risk of developing AMD to return to the baseline level of a never-smoker.6 This long latency reflects the time required for the RPE to clear accumulated lipofuscin and for the choriocapillaris to repair endothelial damage.
- Recalcitrant Risk: Even 15 years after quitting, women in the Nurses' Health Study who had smoked heavily (>25 cigarettes/day) still retained a 2-fold increased risk compared to never-smokers.8 This underscores the imperative of primary prevention—preventing smoking initiation—as the most effective strategy.

3.4 Smoking and Treatment Efficacy
Beyond increasing susceptibility, smoking also degrades the efficacy of treatments for wet AMD. Studies have shown that current smokers require more anti-VEGF injections to achieve disease stability and have poorer visual acuity outcomes compared to non-smokers.15 Smokers present with larger choroidal neovascular lesions and more subretinal fibrosis, rendering the disease more resistant to therapy. This provides a compelling "teachable moment" for clinicians: advising patients that quitting smoking is not just for their lungs, but is an adjuvant therapy necessary to make their eye injections work effectively.
4. Nutritional Defense: The Mediterranean Paradigm
While smoking accelerates retinal destruction, nutrition provides the substrates for retinal defense. Among the various dietary patterns studied, the Mediterranean Diet (MeDi) has emerged with the strongest evidence base for AMD prevention. Unlike reductionist approaches that focus on single nutrients (e.g., vitamin supplements), the MeDi represents a holistic "food matrix" approach, delivering a synergistic combination of antioxidants, anti-inflammatory lipids, and prebiotic fibers.

4.1 The Mediterranean Diet Score and AMD Risk
The protective effects of the MeDi are supported by high-quality meta-analyses and pooled cohort data. The Rotterdam Study and the Alienor Study, two of the most significant European cohorts, pooled their data to investigate the association between MeDi adherence (measured by a 9-point score) and incident advanced AMD.
- Risk Reduction: Participants with high adherence (scores 6–9) exhibited a 41% reduced risk of developing incident advanced AMD compared to those with low adherence (scores 0–3), with a Hazard Ratio (HR) of 0.59 (95% CI: 0.37–0.95).16
- Progression Prevention: A broader meta-analysis of prospective cohort studies confirmed this finding, reporting a pooled Hazard Ratio of 0.77 (95% CI: 0.67–0.88) for disease progression.17 This indicates that even in patients who already have early drusen, shifting to a Mediterranean diet can reduce the likelihood of progressing to blindness by nearly a quarter.
4.2 Differential Effects on AMD Phenotypes
Interestingly, the protection afforded by the MeDi appears to vary by disease subtype, though findings are nuanced.
- Geographic Atrophy (GA): Several analyses, including those from the AREDS cohort, suggest that the protective signal is stronger for Geographic Atrophy than for neovascular AMD. In the AREDS participants, closer adherence to the MeDi was associated with a significantly lower risk of progression to GA (HR 0.79; p=0.004).18 Given the lack of effective treatments for GA until recently, this dietary intervention is of paramount clinical importance.
- Neovascular AMD: Other studies, such as the Alienor study, have found protective associations for neovascular disease as well. The inconsistencies likely arise from the different pathophysiological drivers: GA is driven more by oxidative stress/apoptosis (mitigated by antioxidants in the diet), while NV-AMD is driven by ischemia/angiogenesis (mitigated by vascular-protective lipids).19
4.3 Key Bioactive Components
The efficacy of the MeDi is attributed to specific nutrient groups that target the retina's vulnerabilities:
- Lutein and Zeaxanthin: Found in dark leafy greens (spinach, kale) and egg yolks, these xanthophyll carotenoids are selectively transported to the macula. They form the "macular pigment," which absorbs up to 90% of incident blue light, preventing photochemical damage. They also act as potent quenchers of singlet oxygen. High dietary intake is strongly correlated with reduced risk of progression.2
- Omega-3 Fatty Acids (DHA/EPA): Fatty fish (salmon, mackerel, sardines) are the cornerstone of the MeDi. Docosahexaenoic acid (DHA) is a structural lipid in photoreceptor outer segments, essential for membrane fluidity and signal transduction. Eicosapentaenoic acid (EPA) is the precursor for anti-inflammatory eicosanoids. In the AREDS2 study, participants with the highest intake of omega-3s had a significantly lower risk of late AMD, an effect that persisted even when controlling for supplement use.18
- Polyphenols: Extra virgin olive oil and red wine (consumed in moderation) are rich in polyphenols like oleocanthal and resveratrol. These compounds induce the Nrf2 antioxidant response element in RPE cells, enhancing the expression of detoxification enzymes like heme oxygenase-1.20
- Low Glycemic Index: The MeDi is naturally low in refined carbohydrates. High glycemic diets lead to chronic hyperglycemia, which promotes the formation of Advanced Glycation End-products (AGEs). AGEs accumulate in Bruch’s membrane, cross-linking collagen and reducing the membrane's permeability to nutrients and waste. By avoiding AGE formation, the MeDi helps maintain the structural integrity of the RPE-choroid interface.5

4.4 The Gut-Retina Axis
Emerging science points to a "gut-retina axis" as a mechanism for the MeDi's success. The high fiber content from legumes, fruits, and whole grains promotes a diverse gut microbiome. A healthy microbiome produces short-chain fatty acids (SCFAs) like butyrate, which enter the systemic circulation and downregulate systemic inflammation. Dysbiosis (an imbalance of gut bacteria), often caused by Western diets high in processed foods, has been linked to elevated systemic complement activation, which exacerbates AMD in genetically susceptible hosts.1
5. Physical Activity: Systemic Perfusion and Retinal Resilience
While diet is often discussed in eye clinics, physical activity (PA) is frequently neglected. However, the accumulated evidence suggests that exercise is a powerful, dose-dependent modifier of AMD risk, acting through mechanisms distinct from those of nutrition.
5.1 The Statistical Case for Movement
Sedentary behavior is a risk factor for AMD, while physical activity is protective. A systematic review and meta-analysis of physical activity and AMD risk found compelling protective associations:
- Late AMD Protection: Physical activity was associated with an Odds Ratio of 0.59 (95% CI: 0.49–0.72) for developing late AMD.21 This translates to a 41% reduction in the odds of blindness for active individuals compared to sedentary controls.
- Early AMD: The association with early AMD is also significant but more modest, with an OR of 0.92 (95% CI: 0.86–0.98).21
- Incidence: In a 15-year prospective study, older adults in the highest tertile of physical activity were 79% less likely (OR 0.21) to have incident late AMD compared to the lowest tertile, after adjusting for age.22 While further adjustment for other lifestyle factors attenuated this specific statistic, the trend remains robust across multiple cohorts.
5.2 Intensity and Dose-Response: Is More Better?
A key debate in the literature concerns the intensity of exercise required. Does one need to run marathons, or is walking sufficient? The data supports a "more is better" approach, but with diminishing returns at the extreme end.
- Vigorous Activity: High-intensity exercise appears to confer the greatest benefit. In the National Runners' Health Study, men and women who ran an average of 8 km/day or more had a 54% lower risk of AMD compared to those running less than 2 km/day.23 The relationship was convex, with significant risk reductions appearing at thresholds of 2–4 km/day.
- Walking: Moderate activity is also effective. One study found that increasing the number of "blocks walked per day" was associated with a 30% reduction in the risk of exudative AMD (OR 0.7).24 This is encouraging for elderly populations for whom vigorous running may not be feasible.
- The Plateau Effect: General mortality studies suggest that benefits plateau at 3–5 times the recommended minimum activity guidelines, but there is no evidence of harm (the "U-shaped curve") for retinal health at high levels of exercise.25
5.3 Mechanisms: The Muscle-Eye Connection
How does contracting skeletal muscle protect the retina? The mechanisms are likely pleiotropic, involving vascular, metabolic, and neurotrophic pathways.
- Brain-Derived Neurotrophic Factor (BDNF): Often termed "fertilizer for the brain," BDNF is also critical for the retina. Physical activity stimulates the production of BDNF in skeletal muscle and the brain, raising systemic levels. BDNF crosses the blood-retina barrier and binds to TrkB receptors on retinal ganglion cells and photoreceptors, promoting their survival. In mouse models, exercise increased retinal BDNF protein levels by 20%, and blocking BDNF receptors completely negated the protective effect of exercise against light-induced retinal degeneration.26 This provides a direct molecular link between the treadmill and the photoreceptor.
- Angiogenesis Inhibition: Exercise may act as a physiological "anti-VEGF." In laboratory mice, voluntary exercise reduced the volume of choroidal neovascular lesions by up to 45%.28 This effect is likely mediated by the improved regulation of hypoxia-inducible factors and the reduction of systemic inflammation (e.g., lower CRP levels), which suppresses the angiogenic drive.
- Mitochondrial Quality Control: The RPE relies on mitophagy to clear defective mitochondria. Aging impairs this process, leading to oxidative stress. Exercise has been shown to restore autophagy and mitophagy flux in retinal tissues, effectively "cleaning up" the RPE and preventing the accumulation of lipofuscin.29
- Systemic Perfusion: Exercise improves endothelial function via shear stress-mediated release of nitric oxide. This improves choroidal blood flow, ensuring that the RPE receives adequate oxygen and that waste products are efficiently flushed from Bruch’s membrane.7

6. The Synergistic Effect: Combined Lifestyle Scores
While researchers study risk factors in isolation, patients live them in combination. The most powerful insights come from analyses of "Combined Lifestyle Scores," which aggregate diet, smoking, and physical activity into a single index.
6.1 The "Healthy Lifestyle" Multiplier
The Carotenoids in Age-Related Eye Disease Study (CAREDS) provided a landmark analysis of this synergy. The study tracked women aged 50–74 and scored them on a healthy lifestyle index (healthy diet, regular physical activity, and not smoking).
- 71% Risk Reduction: Women who adhered to all three healthy behaviors had 71% lower odds (OR 0.29) of developing AMD compared to those with low lifestyle scores.31
- Attributable Risk: Population-attributable risk analyses suggest that approximately 25% to 37% of AMD cases could be theoretically prevented if the entire population shifted from a "poor" to an "ideal" lifestyle profile.32
6.2 Interaction with Genetic Susceptibility
A crucial finding for the era of personalized medicine is that lifestyle can buffer genetic risk. In the CAREDS cohort, researchers stratified patients by their genetic risk score (based on CFH and ARMS2 variants).
- High Risk, Bad Habits: Individuals with high genetic risk (e.g., CFH CC genotype) who also had the least healthy lifestyle had an Odds Ratio of 3.34 to 4.63 for AMD compared to low-risk, healthy-living individuals.3
- High Risk, Good Habits: However, high-risk individuals who adopted a healthy lifestyle significantly reduced their absolute risk. While they could not completely eliminate their genetic disadvantage, the adoption of healthy behaviors brought their risk profile much closer to that of the general population. This finding empowers clinicians to tell patients: "Your genes load the gun, but your lifestyle pulls the trigger." Genetic testing, therefore, should not lead to fatalism but should serve as a motivator for aggressive lifestyle optimization.

7. Clinical Guidelines and Public Health Implications
Despite the overwhelming evidence supporting lifestyle interventions, their integration into routine clinical practice remains inconsistent. The disconnect between epidemiological knowledge and clinical implementation represents a major gap in AMD care.
7.1 Barriers to Implementation
Surveys of retina specialists indicate that while most ask about smoking, fewer detail specific dietary changes beyond "eat leafy greens," and fewer still prescribe exercise. Barriers include:
- Time Constraints: In high-volume retina clinics, the focus is often on imaging and injections.
- Lack of Training: Ophthalmologists receive minimal training in nutrition or exercise physiology.
- Reimbursement: Lifestyle counseling is rarely reimbursed at the same level as diagnostic imaging or procedures.

7.2 A Proposed Clinical Pathway
To bridge this gap, a "Lifestyle Prescription" approach is recommended:
- Assess: Quantify smoking status (pack-years) and physical activity (minutes/week) at baseline.
- Prescribe: Provide a written "prescription" for:
- Diet: "Mediterranean Pattern: High fish, olive oil, greens; low sugar/processed food."
- Activity: "Goal: 150 minutes moderate or 75 minutes vigorous activity per week."
- Tobacco: "Referral to cessation hotline/clinic."
- Refer: Utilize multidisciplinary teams. Refer patients with high BMI or metabolic syndrome to dietitians or endocrinologists, framing it as part of their eye care.
- Monitor: Follow up on lifestyle adherence at 6-month intervals, using MPOD scores or simple questionnaires as biomarkers of compliance.
8. Conclusion
The management of Age-Related Macular Degeneration stands at a crossroads. The era of anti-VEGF therapy has saved millions of years of sight, but it treats the smoke, not the fire. The underlying drivers of retinal degeneration—oxidative stress, chronic inflammation, and vascular senescence—are intimately tethered to the way patients live.
This comprehensive review confirms that lifestyle is a primary therapeutic target. A diet rich in Mediterranean staples can reduce the risk of progression by ~40%. Vigorous physical activity can lower the risk of late disease by ~50%. Smoking cessation, while a long road to full recovery, is the single most effective action a patient can take to delay onset. When combined, these factors offer a potential 71% reduction in the risk of this blinding disease.
For the clinician, the message is clear: the conversation about lifestyle is not an optional addendum to care; it is central to the preservation of vision. For the researcher, the challenge is to refine our understanding of the "dose" of these interventions and to elucidate the molecular mechanisms that link muscle, gut, and retina. And for the public, the science offers a message of agency and hope: blindness is not an inevitable consequence of aging, and the power to protect one’s sight lies, to a significant degree, in one’s own hands.

Table 1: Summary of Risk Reductions by Lifestyle Intervention
|
Intervention |
Comparison |
Outcome Measure |
Effect Size (OR/HR) |
Source |
|
Mediterranean Diet |
High vs Low Adherence |
Incident Advanced AMD |
HR 0.59 (41% reduction) |
16 |
|
Mediterranean Diet |
High Adherence |
Progression from Early AMD |
HR 0.77 (23% reduction) |
17 |
|
Physical Activity |
Active vs Sedentary |
Late AMD Incidence |
OR 0.59 (41% reduction) |
21 |
|
Vigorous Running |
>8 km/day vs <2 km/day |
AMD Risk |
RR 0.46 (54% reduction) |
23 |
|
Smoking |
Current vs Never |
AMD Risk (General) |
OR 2.39 - 4.22 (2-4x risk) |
8 |
|
Heavy Smoking |
>40 pack-years |
Geographic Atrophy |
OR 3.43 (3.5x risk) |
10 |
|
Combined Lifestyle |
All Healthy vs None |
AMD Incidence |
OR 0.29 (71% reduction) |
31 |
References
- Modifiable Lifestyle Risk Factors and Strategies for Slowing the Progression of Age-Related Macular Degeneration - PubMed Central, accessed January 7, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC11946629/
- Effect of the Mediterranean Diet on Progression of Dry Form of Age-related Macular Degeneration | In Vivo, accessed January 7, 2026, https://iv.iiarjournals.org/content/37/4/1809
- Joint Associations of Diet, Lifestyle, and Genes with Age-Related ..., accessed January 7, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC4714866/
- The interplay of autophagy and oxidative stress in the pathogenesis and therapy of retinal degenerative diseases - PMC - PubMed Central - NIH, accessed January 7, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC8725349/
- Antioxidative Role of Heterophagy, Autophagy, and Mitophagy in the Retina and Their Association with the Age-Related Macular Degeneration (AMD) Etiopathogenesis - MDPI, accessed January 7, 2026, https://www.mdpi.com/2076-3921/12/7/1368
- Tobacco and age-related macular degeneration - Canada.ca, accessed January 7, 2026, https://www.canada.ca/en/health-canada/services/health-concerns/tobacco/legislation/tobacco-product-labelling/smoking-related-macular-degeneration.html
- Exercise Improves Retinal Health | Mahajan Laboratories - Stanford University, accessed January 7, 2026, https://mahajanlab.stanford.edu/news/exercise-improves-retinal-health
- Smoking and Age-Related Macular Degeneration: Review and Update - PMC - NIH, accessed January 7, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC3866712/
- Smoking and age related macular degeneration: the number of pack ..., accessed January 7, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC1856879/
- the number of pack years of cigarette smoking is a major determinant of risk for both geographic atrophy and choroidal neovascularisation | Tobacco Control, accessed January 7, 2026, https://tobaccocontrol.bmj.com/content/15/2/77
- Global burden of smoking-associated age-related macular degeneration: Spatiotemporal trends from 1990 to 2021 and projections to 2040 - Tobacco Induced Diseases, accessed January 7, 2026, https://www.tobaccoinduceddiseases.org/Global-burden-of-smoking-associated-age-related-macular-degeneration-Spatiotemporal,205665,0,2.html
- Smoking-Attributable Age-Related Macular Degeneration Vision Loss in China: 1990–2021 Trends and 2040 Projections | TVST, accessed January 7, 2026, https://tvst.arvojournals.org/article.aspx?articleid=2810975
- Review Article Smoking and Age-Related Macular Degeneration - DADUN, accessed January 7, 2026, https://dadun.unav.edu/server/api/core/bitstreams/c318550d-79b9-4a00-9df6-2d2e351ee3a3/content
- Smoking and the risk of age-related macular degeneration: a meta-analysis - PubMed, accessed January 7, 2026, https://pubmed.ncbi.nlm.nih.gov/18652983/
- Smoking and treatment outcomes of neovascular... : British Journal of Ophthalmology - Ovid, accessed January 7, 2026, https://www.ovid.com/journals/bjop/fulltext/10.1136/bjophthalmol-2019-314849~smoking-and-treatment-outcomes-of-neovascular-age-related
- Mediterranean Diet and Incidence of Advanced Age-Related ..., accessed January 7, 2026, https://pubmed.ncbi.nlm.nih.gov/30114418/
- Mediterranean Diet on Development and Progression of Age-Related Macular Degeneration: Systematic Review and Meta-Analysis of Observational Studies - MDPI, accessed January 7, 2026, https://www.mdpi.com/2072-6643/17/6/1037
- Adherence to the Mediterranean Diet and Progression to Late Age-Related Macular Degeneration in the Age-Related Eye Disease Studies 1 and 2 - PubMed, accessed January 7, 2026, https://pubmed.ncbi.nlm.nih.gov/32348832/
- Mediterranean diet as a modifiable risk factor for age-related macular degeneration: A systematic review and meta-analysis - PubMed Central, accessed January 7, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC11025595/
- Effect of the Mediterranean Diet (MeDi) on the Progression of Retinal Disease: A Narrative Review - MDPI, accessed January 7, 2026, https://www.mdpi.com/2072-6643/16/18/3169
- Physical Activity and Age-related Macular Degeneration: A Systematic Literature Review and Meta-analysis - PubMed, accessed January 7, 2026, https://pubmed.ncbi.nlm.nih.gov/28549846/
- Physical Activity and the 15-Year Incidence of Age-Related Macular Degeneration | IOVS, accessed January 7, 2026, https://iovs.arvojournals.org/article.aspx?articleid=2212634
- Prospective Study of Incident Age-Related Macular Degeneration in Relation to Vigorous Physical Activity during a 7-Year Follow-up - NIH, accessed January 7, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC4090325/
- Physical activity and the 15‐year cumulative incidence of age‐related macular degeneration: the Beaver Dam Eye Study - PMC - NIH, accessed January 7, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC1857544/
- Leisure Time Physical Activity and Mortality: A Detailed Pooled Analysis of the Dose-Response Relationship - PMC - PubMed Central, accessed January 7, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC4451435/
- Aerobic Exercise Protects Retinal Function and Structure from Light-Induced Retinal Degeneration | Journal of Neuroscience, accessed January 7, 2026, https://www.jneurosci.org/content/34/7/2406.short
- Aerobic Exercise Protects Retinal Function and Structure from Light-Induced Retinal Degeneration - PMC - NIH, accessed January 7, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC3921416/
- Exercise Can Help Prevent or Slow Macular Degeneration, accessed January 7, 2026, https://www.macular.org/about-macular-degeneration/what-is-macular-degeneration/reduce-your-risk/exercise
- Autophagy Protects the Retina from Light-induced Degeneration - PMC, accessed January 7, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC3597791/
- Autophagy in Age-Related Macular Degeneration: A Regulatory Mechanism of Oxidative Stress - PMC - PubMed Central, accessed January 7, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC7429811/
- Healthy lifestyle can reduce AMD risk as much as three-fold, accessed January 7, 2026, https://www.aao.org/education/editors-choice/healthy-lifestyle-can-reduce-amd-risk-as-much-thre
- Association of a Healthy Lifestyle With All-Cause and Cause-Specific Mortality Among Individuals With Probable Sarcopenia: Population-Based Cohort Study - PubMed Central, accessed January 7, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC12303552/
- Age-Related Macular Degeneration Preferred Practice Pattern - American Academy of Ophthalmology, accessed January 7, 2026, https://www.aao.org/Assets/f832e5ac-c047-4d1c-bdab-c5e52173623d/638760137410500000/age-related-macular-degeneration-ppp-pdf
- What Advice Is Currently Given to Patients with Age-Related Macular Degeneration (AMD) by Eyecare Practitioners, and How Effective Is It at Bringing about a Change in Lifestyle? A Systematic Review - PMC - PubMed Central, accessed January 7, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC9658969/
- AMD Commissioning Guidance Evidence Base May 2024 - The Royal College of Ophthalmologists, accessed January 7, 2026, https://www.rcophth.ac.uk/wp-content/uploads/2021/08/AMD-Commissioning-Guidance-Evidence-Base-2024.pdf
{kind=link}
Leave a comment
This site is protected by hCaptcha and the hCaptcha Privacy Policy and Terms of Service apply.