Comprehensive Review of Physical Activity and Age-Related Macular Degeneration: Risk, Progression, and Recommended Protocols
1. Introduction: The Intersection of Ocular Health and Systemic Physiology
Age-Related Macular Degeneration (AMD) stands as a predominant cause of irreversible visual impairment in the developed world, presenting a burgeoning public health crisis as global demographics shift toward an aging population. The disease pathology, characterized by the progressive degeneration of the macula—the central portion of the retina responsible for high-acuity vision—manifests primarily in two forms: non-neovascular (dry) AMD, defined by the accumulation of extracellular deposits known as drusen and atrophy of the retinal pigment epithelium (RPE); and neovascular (wet) AMD, marked by pathological choroidal neovascularization (CNV) and vascular leakage. Current projections estimate that the number of individuals affected by AMD globally will rise to 288 million by the year 2040, imposing a profound burden on healthcare systems and individual quality of life.1
 While therapeutic advancements, particularly anti-vascular endothelial growth factor (anti-VEGF) agents, have transformed the management of neovascular AMD, these treatments are palliative rather than curative, addressing late-stage complications without halting the underlying degenerative processes. Furthermore, for the vast majority of patients diagnosed with early or intermediate dry AMD, no effective medical treatments exist to prevent progression to advanced stages, aside from specific antioxidant formulations (AREDS) which offer only modest risk reduction. This therapeutic lacuna necessitates a paradigm shift toward identifying modifiable lifestyle factors that can influence disease trajectory.
While therapeutic advancements, particularly anti-vascular endothelial growth factor (anti-VEGF) agents, have transformed the management of neovascular AMD, these treatments are palliative rather than curative, addressing late-stage complications without halting the underlying degenerative processes. Furthermore, for the vast majority of patients diagnosed with early or intermediate dry AMD, no effective medical treatments exist to prevent progression to advanced stages, aside from specific antioxidant formulations (AREDS) which offer only modest risk reduction. This therapeutic lacuna necessitates a paradigm shift toward identifying modifiable lifestyle factors that can influence disease trajectory.

Among modifiable behaviors, Physical Activity (PA) has emerged as a critical, yet historically underutilized, intervention target. Unlike pharmaceutical approaches that target specific molecular pathways, physical activity exerts pleiotropic effects on systemic physiology—modulating inflammation, oxidative stress, vascular endothelial function, and neurotrophic factor expression—all of which are implicated in AMD pathogenesis. Recent epidemiological evidence, ranging from large-scale longitudinal cohorts to Mendelian randomization studies, suggests a robust inverse relationship between physical activity and AMD risk. However, the literature reveals complex nuances regarding the intensity of exercise required, the differential impact on disease onset versus progression, and the modifying roles of genetics and gender.

This report provides an exhaustive synthesis of the current evidence base linking physical activity to AMD. It critically evaluates epidemiological data on incidence and progression, dissects the biological mechanisms conferring retinal protection, analyzes the profound impact of fear of falling (FoF) on patient mobility, and delineates evidence-based protocols for clinical intervention. By integrating findings from diverse global cohorts—including the National Runners’ Health Study, the Blue Mountains Eye Study, and the E3 Consortium—this review aims to provide a definitive reference for leveraging physical activity in the management of macular degeneration.
2. Epidemiological Evidence: Physical Activity and the Incidence of AMD
The epidemiological landscape regarding physical activity and AMD incidence is vast, characterized by varying methodologies and population demographics. A synthesis of these studies reveals a consistent signal: physical activity is a potent protective factor, though its efficacy is influenced by intensity, dose, and specific demographic variables.

2.1 Vigorous Activity and Dose-Response: The National Runners’ Health Study
One of the most compelling datasets elucidating the relationship between exercise intensity and AMD risk comes from the National Runners’ Health Study. This prospective analysis of 29,532 men and 12,176 women, followed for an average of 7.7 years, provides a unique window into the effects of vigorous physical activity—specifically running—on ocular health.1
The study established a significant, inverse dose-response relationship between the volume of running and the incidence of clinically diagnosed AMD. This association persisted even after rigorous adjustment for potential confounders, including body mass index (BMI), cardiorespiratory fitness, and cigarette smoking history. The data indicates that the protective benefits of exercise are not merely a proxy for a generally healthy lifestyle but are driven by the specific metabolic and physiological adaptations associated with vigorous activity.

Quantitative Risk Reductions:
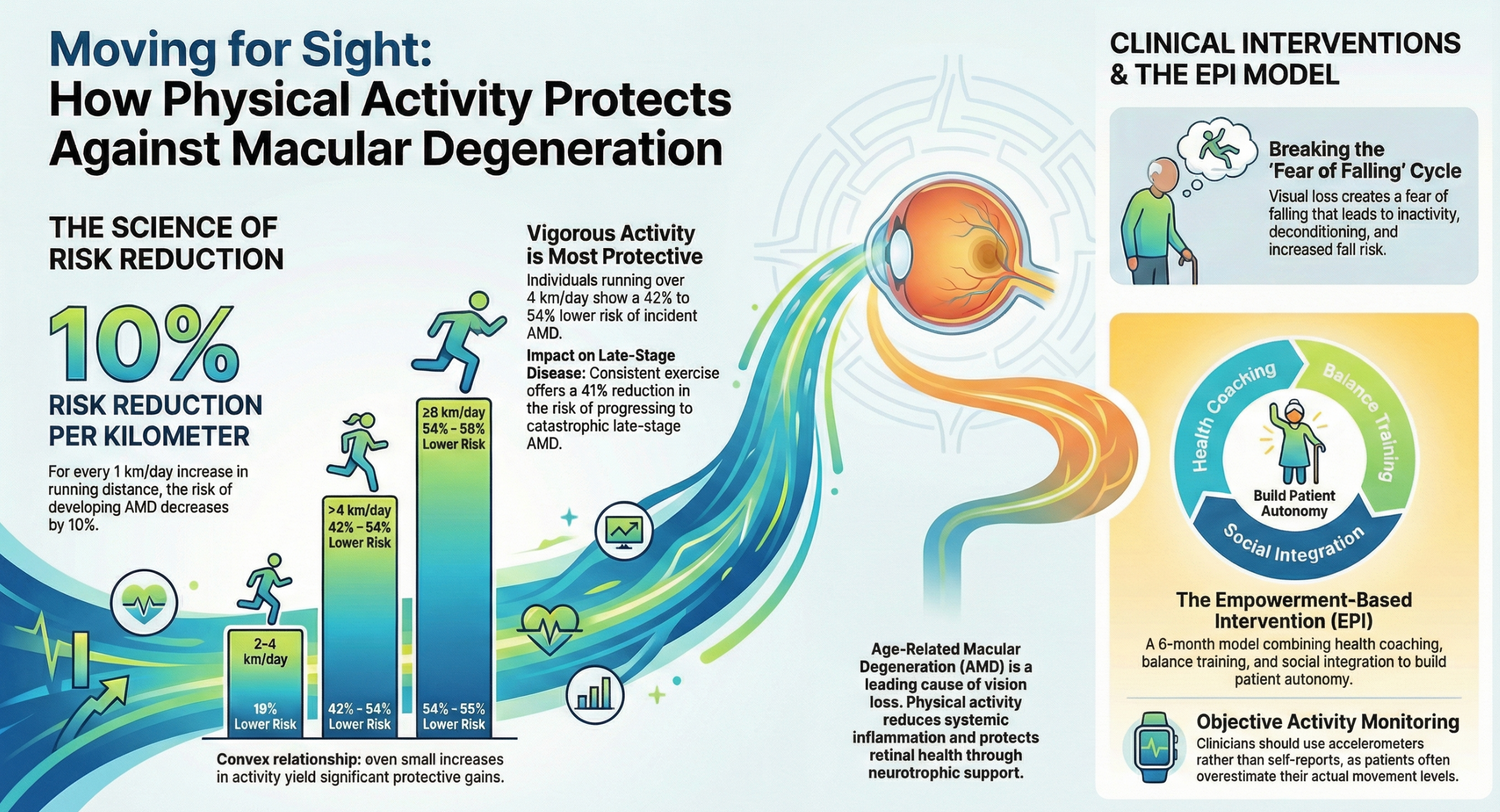
- Linear Decrement: The relative risk for developing AMD decreased by approximately 10% for every 1 kilometer per day (km/d) increment in average running distance.1
- Threshold Effects: The study identified distinct risk strata based on daily running distance, using those running less than 2 km/d as the reference group:
- 2–4 km/d: Individuals in this category exhibited a 19% lower adjusted risk of incident AMD.
- >4 km/d: Runners exceeding this threshold demonstrated a 42% to 54% lower adjusted risk.
- ≥8 km/d: The highest volume group showed the most profound protection, with a 54% to 59% reduction in risk, depending on whether BMI was included in the adjustment model.1
The Convex Nature of Protection:
The statistical analysis revealed the relationship to be "convex," implying that the steepest gains in risk reduction are achieved during the initial increases in activity. Specifically, the transition from running <2 km/d to 2 km/d yielded a statistically significant 36% risk reduction ($P=0.04$). Further increasing distance from the 2–4 km/d range to >4 km/d yielded additional significant benefits ($P=0.03$). This suggests that while elite levels of exercise offer maximum protection, substantial public health benefits can be realized by moving sedentary individuals into moderate vigorous activity brackets.1

Independence from Cardiorespiratory Fitness:
A critical insight from this cohort was the distinction between exercise performance and exercise volume. While 10-km race times (a proxy for cardiorespiratory fitness) were moderately correlated with running distance, fitness itself was not independently associated with AMD risk when adjusted for distance run. This implies that the total energy expenditure and the cumulative physiological stimulus of the activity, rather than the athlete's speed or conditioning level, are the primary drivers of retinal protection.1
2.2 Longitudinal Cohorts and Age-Specific Nuances
While the runners' cohort emphasizes vigorous activity, general population studies provide essential context regarding age, gender, and the severity of disease prevented.
The Blue Mountains Eye Study (BMES):
In this 15-year prospective Australian study, the relationship between physical activity and AMD was found to be heavily influenced by age and adjustment for systemic comorbidities. Among adults aged 75 years and older, those in the highest tertile of physical activity were 79% less likely to develop incident late AMD compared to the lowest tertile in age-adjusted models (OR 0.21; 95% CI 0.05–0.95).1
However, the robustness of this association wavered under multivariate adjustment. When potential mediators such as BMI, smoking status, fish consumption, and white cell count (a marker of systemic inflammation) were included in the model, the association lost statistical significance (OR 0.26; 95% CI 0.06–1.28).1 This loss of significance is scientifically illuminating; it suggests that physical activity does not act on the retina in isolation. Instead, its protective effects are likely mediated through these very pathways—by reducing systemic inflammation, managing weight, and correlating with better dietary habits. Therefore, while the direct statistical link weakened, the practical implication remains that physical activity is a regulator of the risk factors that drive AMD. Notably, this study found no significant association between physical activity and the incidence of early AMD, nor did it find protection for individuals under the age of 75.1
The Melbourne Collaborative Cohort Study:
This study introduced a gender-dimorphic perspective to the evidence base. Analyzing data from over 20,000 participants, researchers found no significant association between total recreational physical activity and AMD risk for the cohort as a whole. However, when stratified by sex and intensity, a specific protective effect emerged for women. Frequent vigorous exercise (defined as ≥3 times/week) was associated with a 22% decrease in the odds of intermediate AMD in women (OR 0.78; 95% CI 0.64–0.96).1 No such association was found in men.
This finding aligns with other data, such as the Tromsø Study, which also observed female-specific protection. The reasons for this gender disparity remain speculative but may involve interactions between exercise-induced metabolic changes and post-menopausal hormonal profiles, or differences in the baseline inflammatory status between aging men and women.1
2.3 Causal Inference: The Role of Mendelian Randomization
A persistent challenge in observational epidemiology is establishing causality. Does physical activity prevent AMD, or does the visual impairment from early, undiagnosed AMD lead to reduced physical activity (reverse causality)? To address this, Zhou et al. (2025) utilized Mendelian randomization (MR), a method that uses genetic variants associated with physical activity as instrumental variables to infer causality, thereby bypassing confounding and reverse causation issues.1
Key Findings from MR Analysis:
- Causal Link Confirmed: The study provided strong genetic evidence that moderate-to-vigorous physical activity (MVPA) is causally associated with a reduced risk of AMD. The odds ratio derived from the genetic analysis was 0.77 (95% CI 0.66–0.89), indicating a substantial protective effect.1
- Sedentary Behavior: Interestingly, the study found no causal link between genetically determined sedentary behaviors (such as sitting at work or commuting) and AMD risk. However, leisure screen time showed a non-significant trend toward increased risk.
This genetic evidence is pivotal. It confirms that the associations observed in longitudinal cohorts are not merely artifacts of healthier people having better vision, but that increasing physical activity creates biological conditions that actively suppress the development of macular degeneration.1
2.4 The Beijing Eye Study: Cultural and Regional Variations
In contrast to the strong associations found in Western populations, the Beijing Eye Study reported only a marginally significant association between physical activity and AMD prevalence ($p=0.04$).1 This association was notably weaker than that found for diabetic retinopathy ($p=0.009$).
This discrepancy highlights the potential influence of genetic background, environmental exposures, and cultural lifestyle differences on disease etiology. For instance, the types of physical activity common in this cohort (e.g., walking, Tai Chi) may differ in intensity from the vigorous running or gym-based exercises often measured in Western studies. Additionally, the baseline prevalence of metabolic risk factors in the Beijing cohort may alter the relative importance of physical activity as a protective mechanism.1
2.5 Meta-Analytic Synthesis
Aggregating these diverse findings, a comprehensive meta-analysis by McGuinness et al. (2017) synthesized data from nine studies involving over 38,000 participants. This analysis concluded that physical activity is associated with lower odds of both early AMD (OR 0.92) and late AMD (OR 0.59).1 The stronger protective effect for late-stage disease (41% risk reduction) versus early-stage disease (8% risk reduction) suggests that physical activity may be particularly effective in preventing the catastrophic progression to neovascularization or geographic atrophy, potentially by maintaining choroidal perfusion and limiting chronic inflammation.
3. Disease Progression: Does Activity Halt the Slide?
A critical clinical question is whether physical activity can slow the worsening of AMD once the disease process has begun. The evidence here suggests a nuanced distinction between preventing incidence (the onset of early disease) and preventing progression (the transition from early to late disease).

The E3 Consortium Multi-Cohort Analysis:
This massive study, pooling longitudinal data from 14,630 adults across seven European and Australian cohorts, utilized Markov multistate models to rigorously track transitions between disease states.1 The results revealed a "threshold effect" for protection:
- Incidence of Early AMD: High levels of physical activity were significantly protective against the transition from "No AMD" to "Early AMD." Individuals with low-to-moderate activity had a 1.19-fold increased risk (HR 1.19; $P=0.04$) of developing early signs of the disease compared to highly active individuals.1
- Progression to Late AMD: However, physical activity levels were not significantly associated with the transition from "Early AMD" to "Late AMD".1
| Study or Cohort Name | Population Description | Sample Size | Physical Activity Metric | Key Findings | Risk Reduction or Odds Ratio | Disease Stage Impact |
| Meta-analysis by McGuinness et al. (2017) | Synthesis of nine prospective and cross-sectional studies | Over 38,000 | General physical activity | Demonstrated a stronger protective effect for late-stage disease compared to early-stage disease. | Early AMD: OR 0.92 (8% reduction); Late AMD: OR 0.59 (41% reduction) | Early and Late AMD |
| National Runners’ Health Study | Prospective analysis of men and women | 29,532 men and 12,176 women | Daily running distance ( $km/d$ ) | Significant inverse dose-response relationship; protection is likely driven by metabolic adaptations to vigorous activity. | 10% reduction per $km/d$ ; 42% to 54% reduction for $>4$ $km/d$ ; 54% to 59% reduction for $\ge 8$ $km/d$ | Incident AMD (onset) |
| Mendelian Randomization Analysis (Zhou et al. 2025) | Genetic analysis using instrumental variables | Not in source | Moderate-to-vigorous physical activity (MVPA) | Confirmed a causal link between MVPA and reduced AMD risk; no causal link was found for sedentary behavior. | OR 0.77 (23% risk reduction) | AMD risk (causality) |
| Blue Mountains Eye Study (BMES) | Adults aged 75 years and older in Australia | Not in source | Tertiles of physical activity | Highest activity tertile was significantly less likely to develop late AMD, though association weakened after multivariate adjustment. | OR 0.21 (79% less likely) in age-adjusted models | Late AMD (No association with early AMD) |
| Melbourne Collaborative Cohort Study | Participants stratified by sex and intensity | Over 20,000 | Frequent vigorous exercise ( $\ge 3$ times/week) | Gender-specific protective effect found specifically in women. | OR 0.78 (22% decrease in odds for women) | Intermediate AMD |
| E3 Consortium Multi-Cohort Analysis | Pooled data from seven European and Australian cohorts | 14,630 adults | Physical activity levels (Markov multistate models) | Protective against the transition from No AMD to Early AMD; no significant effect on the transition from Early to Late AMD. | Low-to-moderate activity: 1.19-fold increased risk (HR 1.19) compared to high activity | Transition to Early AMD only |
| NHANES Study | US adults cross-sectional study | Not in source | MVPA measured via visual acuity control | Participants with late AMD engaged in significantly less activity, primarily attributed to vision loss. | 50% less MVPA compared to those without AMD | Late AMD |
| Beijing Eye Study | Regional population in China | Not in source | Physical activity (e.g., walking, Tai Chi) | Only a marginally significant association was observed, which is weaker than findings in Western cohorts. | $p=0.04$ (marginally significant) | AMD prevalence |
The "Metabolic Rescue" Hypothesis:
This finding implies that physical activity is most effective as a primary preventative measure. In the healthy retina, the systemic benefits of exercise—improved lipid profiles, reduced oxidative stress, and enhanced perfusion—may be sufficient to maintain RPE homeostasis and prevent the initial accumulation of drusen. However, once the pathological cascade is established (early AMD), the disease may become driven by local ocular mechanisms (e.g., complement activation, local oxidative stress, RPE senescence) that are less responsive to systemic exercise-induced modulation.
This does not negate the value of exercise for patients with early AMD. Given the systemic comorbidities often associated with AMD (cardiovascular disease, hypertension), physical activity remains crucial for overall health and mortality reduction. Furthermore, while the E3 study did not find statistical significance for late AMD progression, other meta-analyses (like McGuinness et al.) did find strong associations with prevalent late AMD, suggesting that survival bias or differences in study design may account for the discrepancy.

4. Mechanisms of Action: How Exercise Protects the Retina
The protective effects of physical activity on the retina are biologically plausible and are likely mediated through a complex interplay of systemic and local mechanisms. The retina is a high-energy tissue with the greatest metabolic demand per unit weight in the human body, making it uniquely susceptible to oxidative stress and perfusion deficits.
4.1 Systemic Inflammation and C-Reactive Protein (CRP)
Chronic, low-grade systemic inflammation is a central driver of AMD pathogenesis. Elevated levels of C-reactive protein (CRP), a marker of systemic inflammation, are consistently associated with increased AMD risk. Physical activity acts as a potent modulator of this inflammatory state.

Research by Subhi et al. demonstrated that in patients with neovascular AMD, physical activity was independently associated with significantly lower CRP levels ($P=0.009$).1 Physically active patients exhibited a median CRP of 1.6 mg/L, compared to 2.1 mg/L in inactive patients. Crucially, the study found that the presence of neovascular AMD itself did not contribute to elevated CRP when physical activity was accounted for. This suggests that the "inflammatory profile" often attributed to AMD patients may largely be a consequence of their sedentary lifestyle—driven by visual impairment—rather than the disease pathology itself.1
Mechanism: Skeletal muscle acts as an endocrine organ. During contraction, muscles release myokines (such as IL-6) which, in the context of exercise, exert anti-inflammatory effects by inhibiting the production of TNF-alpha and stimulating the release of anti-inflammatory cytokines like IL-10 and IL-1ra.
4.2 Oxidative Stress and Mitochondrial Function
The RPE is tasked with phagocytosing shed photoreceptor outer segments, a process that generates significant oxidative stress. Mitochondria in the RPE are essential for generating the ATP required for this high metabolic turnover.
- Antioxidant Defense: Exercise upregulates endogenous antioxidant defense systems, including superoxide dismutase (SOD) and glutathione peroxidase (GPx), enhancing the retina's capacity to neutralize reactive oxygen species (ROS).2
- Mitochondrial Health: Physical activity promotes mitochondrial biogenesis and efficiency. In the RPE, efficient mitochondrial function is critical for preventing the accumulation of lipofuscin and other toxic byproducts that constitute drusen. Reductive carboxylation in mitochondria has been suggested as a pathway supporting RPE resilience against oxidative damage.4
 4.3 Neuroprotection via Brain-Derived Neurotrophic Factor (BDNF)
4.3 Neuroprotection via Brain-Derived Neurotrophic Factor (BDNF)
BDNF is a neurotrophin essential for the survival and maintenance of neurons. The retina, embryologically an extension of the brain, is responsive to neurotrophic support.
- Exercise Induction: Physical activity is a well-established inducer of systemic and central BDNF expression.
- Retinal Protection: Animal models have shown that aerobic exercise increases retinal BDNF protein levels by approximately 20%.5 This upregulation has been linked to the protection of retinal structure and function against light-induced degeneration.5 Blocking BDNF receptors (TrkB) negates the protective effects of exercise, identifying BDNF signaling as a critical pathway for exercise-induced retinal neuroprotection.6
4.4 Choroidal Perfusion
The choroid provides the blood supply to the outer retina and RPE. While some studies on isometric exercise did not show significant differences in choroidal blood flow regulation between AMD patients and controls 8, aerobic exercise is generally known to improve endothelial function and vascular reactivity. Maintaining adequate choroidal perfusion is vital for nutrient delivery and waste removal from the RPE, and exercise-induced improvements in cardiovascular health likely translate to better ocular perfusion pressure and vascular health.10
5. The Reality of Activity in the AMD Population
Despite the clear benefits of physical activity, the AMD population is characterized by significantly reduced activity levels, creating a deleterious cycle of disease, disability, and sedentarism.
5.1 The Discrepancy Between Objective and Self-Reported Activity
Assessing physical activity in visually impaired populations is fraught with measurement error. A study by Zult et al. highlighted a significant discordance between what AMD patients report doing and what they actually do.

- Objective Reality: When measured using accelerometers, healthy controls engaged in 33–34% more moderate-to-vigorous physical activity (MVPA) than AMD patients (both with and without vision loss).1
- Subjective Illusion: Self-reported questionnaires (GPAQ) failed to detect significant differences between the groups.
- Under-Reporting: Interestingly, while all groups under-reported their activity compared to accelerometers, healthy controls under-reported their MVPA significantly more than AMD patients. This implies that relying on self-reports may mask the true extent of the activity deficit in the AMD population.1
 5.2 Activity Patterns and Fragmentation
5.2 Activity Patterns and Fragmentation
It is not just the total volume of activity that suffers, but the pattern of accumulation. Research by the ENGAGE group using accelerometry data has shown that visual field damage is associated with "activity fragmentation"—short bursts of activity followed by rest—rather than sustained movement.1 This fragmentation is a marker of functional decline, higher fatigability, and poorer physiological reserve.
5.3 The Impact of Vision Loss on Movement
The NHANES study revealed that participants with late AMD engaged in 50% less MVPA compared to those without AMD.11 Importantly, when visual acuity was controlled for in the statistical models, the association between AMD and reduced activity was attenuated. This indicates that it is the loss of vision itself—and the associated difficulties with navigation, balance, and hazard detection—that acts as the primary barrier to activity, rather than the systemic nature of the disease directly draining energy levels.11

6. The Psychological Barrier: Fear of Falling (FoF)
The most significant non-physiological barrier to physical activity in the AMD population is the Fear of Falling (FoF). This psychological phenomenon acts as a potent mediator between visual impairment and sedentary behavior, creating a "vicious cycle" of decline.
6.1 The Vicious Cycle of Inactivity
- Visual Impairment: AMD reduces depth perception, contrast sensitivity, and visual field integrity. This increases the actual risk of falls by 2- to 8-fold compared to visually normal peers.1
- Fear of Falling (FoF): Aware of this risk, patients develop a protective, yet maladaptive, psychological response: a pervasive fear of falling.
- Activity Restriction: To mitigate anxiety and avoid potential falls, individuals intentionally restrict their movement, avoiding travel outside the home and reducing engagement in daily activities.1
- Physical Deconditioning: This self-imposed sedentary behavior leads to muscle atrophy, reduced proprioception, and poorer balance.
- Increased Fall Risk: Paradoxically, this deconditioning increases the actual risk of falls, reinforcing the fear and perpetuating the cycle.1
Research indicates that older adults with high FoF are more likely to transition to dependence in daily activities and suffer from social isolation and depression.1 Addressing FoF is therefore a prerequisite for any successful physical activity intervention in this population. Programs that fail to address the psychological component of mobility restriction are likely to fail.

7. Recommended Protocols and Interventions
Given the established benefits of physical activity for AMD risk reduction and the significant barriers faced by patients, clinical management must evolve beyond ocular injections and supplements to include prescriptive physical activity. Effective interventions must be holistic, addressing the physiological need for exercise, the safety of the environment, and the psychological barrier of fear.
7.1 The Empowerment-Based Physical Activity Intervention (EPI) Model
A promising, evidence-based protocol identified in the literature is the Empowerment-Based Physical Activity Intervention (EPI), designed specifically for older adults with advanced dry AMD.1 This mixed-methods approach moves beyond simple exercise prescription to address the root causes of inactivity.
Core Components of the EPI Model:
- Reflective Equilibrium Approach: This philosophy combines "top-down" expertise (researchers designing safety protocols) with "bottom-up" participant power (patients choosing activities that align with their lifestyle goals). This autonomy is crucial for long-term adherence.
- Health Coaching: The protocol includes three individual coaching sessions (Start, Month 4, Month 6) utilizing motivational interviewing techniques. The goal is to build self-efficacy, reframe negative beliefs about capability, and set personalized goals.
- Social Integration: To combat the isolation associated with AMD, the program includes post-exercise social gatherings with refreshments. This facilitates peer support and knowledge exchange.
- Duration: A 6-month structured program is recommended to establish habit formation.

Specific Activities within EPI:
- Group Balance Training: Conducted twice weekly for one hour. The curriculum focuses specifically on strength, movement, and flexibility exercises designed to improve stability and directly target fall risk.
- Adapted Sports: Activities like adapted table tennis are used to promote hand-eye coordination, reaction time, and social engagement without the pressure of high-performance competition.
- Sustainability Transition: In the later stages of the intervention, participants are introduced to municipal drop-in gyms. Researchers educate gym staff on the specific support needs of visually impaired clients, facilitating a smooth transition from a clinical setting to community-based activity.
 7.2 Environmental and Safety Interventions
7.2 Environmental and Safety Interventions
Modifying the physical environment is a first-line strategy to enable safe mobility and reduce the actual risk of falls.
- Occupational Therapist-Led Assessments: Evidence suggests that home safety assessments are significantly more effective when led by occupational therapists (OTs) rather than non-specialists. OTs can expertly identify hazards (e.g., loose rugs, poor lighting) and recommend modifications.1
- Hazard Modification: Standard protocols include removing trip hazards, improving ambient lighting, installing grab bars, and enhancing contrast on stairs/edges to compensate for reduced contrast sensitivity.
- Limitations: While environmental modification reduces falls, studies suggest it does not necessarily increase physical activity levels on its own. It makes the home safer but does not motivate the patient to move more; thus, it must be paired with behavioral interventions.1

7.3 Behavioral and Exercise Strategies
- Exercise Programs: The US Preventive Service Task Force (USPSTF) recommends exercise for fall prevention in the elderly with moderate certainty. For AMD patients, programs must be adapted to accommodate visual deficits (e.g., using auditory cues, high-contrast equipment).1
- The Alexander Technique: While theoretically sound for improving movement quality, trials found this technique was not useful for preventing falls or reducing FoF in visually impaired older adults over a 12-month period, suggesting that more direct strength and balance training is required.1

7.4 Summary of Clinical Recommendations
Based on the synthesis of epidemiological data and intervention studies, the following clinical protocols are recommended for the management of patients with or at risk of AMD:

|
Domain |
Recommendation |
Rationale & Evidence |
|
Assessment |
Use objective accelerometry (or validated wearable devices) to assess baseline activity. Do not rely solely on self-reports. |
Patients underestimate their inactivity; self-reports fail to capture the significant deficit compared to healthy controls.1 |
|
Exercise Type |
Prioritize Moderate-to-Vigorous Physical Activity (MVPA). |
MVPA (e.g., brisk walking, running) shows the strongest causal link to reduced AMD risk in genetic and longitudinal studies.1 |
|
Dosing |
Aim for >150 minutes/week of moderate activity. Ideally, encourage 2–4 km/day of walking/running. |
Risk reduction is incremental. Even modest amounts (2 km/day) show significant benefit (36% reduction), with greater benefits at higher volumes.1 |
|
Fall Prevention |
Refer for OT-led home safety assessments combined with balance training. |
OT assessments are proven to reduce falls; balance training addresses the physical deficit caused by deconditioning.1 |
|
Behavioral Support |
Screen for Fear of Falling (FoF) and implement Health Coaching. |
FoF is the primary mediator of activity restriction. Addressing it through coaching increases self-efficacy and adherence.1 |
|
Sustainability |
Integrate patients into community-based adapted sports or municipal gyms with trained staff. |
Sustainable activity requires social support and accessible facilities that understand visual impairment needs.1 |

8. Conclusion
The relationship between physical activity and Age-Related Macular Degeneration is characterized by robust evidence supporting protection against disease onset and nuanced evidence regarding disease progression. High levels of physical activity, particularly vigorous exercise, are causally linked to a reduced risk of developing early AMD, likely through the modulation of systemic inflammation (CRP), oxidative stress, and neurotrophic support (BDNF). While PA may not halt the progression to late-stage AMD once the disease is established, it remains a critical intervention for preserving remaining visual function, reducing comorbidity, and maintaining quality of life.
However, the AMD population faces unique and profound barriers to activity, primarily the fear of falling, which leads to a self-perpetuating cycle of inactivity and functional decline. Clinical management of AMD must therefore evolve beyond the prescription of ocular injections and antioxidant supplements to include prescriptive, supported physical activity. Effective interventions must be holistic—integrating environmental safety (OT-led modifications) with empowerment-based behavioral coaching and adapted balance training. By addressing both the physiological need for exercise and the psychological barrier of fear, clinicians can significantly improve the health trajectory of individuals living with macular degeneration.









Frequently Asked Questions (FAQs)
How does exercise biologically protect the retina from degeneration?
Exercise biologically protects the retina through a complex interplay of systemic and local mechanisms that address the high metabolic demands and vulnerabilities of retinal tissue. These protective effects are driven by four primary biological pathways:
- Modulating Systemic Inflammation: Chronic, low-grade inflammation is a major driver of Age-Related Macular Degeneration (AMD) pathogenesis, but physical activity acts as a potent modulator that significantly lowers levels of C-reactive protein (CRP), a key inflammatory marker. During physical exertion, skeletal muscles act as an endocrine organ by releasing myokines like IL-6, which inhibit the production of inflammatory TNF-alpha and stimulate beneficial anti-inflammatory cytokines such as IL-10 and IL-1ra.
- Reducing Oxidative Stress and Boosting Mitochondrial Function: The retinal pigment epithelium (RPE) faces massive oxidative stress because it constantly clears shed photoreceptor outer segments. Exercise helps combat this by upregulating endogenous antioxidant defenses, such as superoxide dismutase (SOD) and glutathione peroxidase (GPx), which enhance the retina's ability to neutralize harmful reactive oxygen species (ROS). Additionally, physical activity promotes mitochondrial biogenesis and efficiency in the RPE, which is critical for preventing the accumulation of toxic byproducts like lipofuscin that form drusen.
- Providing Neuroprotection via Brain-Derived Neurotrophic Factor (BDNF): Because the retina is embryologically an extension of the brain, it is highly responsive to neurotrophic support. Aerobic exercise is a well-established inducer of systemic and central BDNF expression, and studies in animal models show it increases retinal BDNF protein levels by approximately 20%. This upregulation actively protects retinal structure and function from light-induced degeneration, a benefit that is entirely negated if BDNF receptors (TrkB) are blocked.
- Improving Choroidal Perfusion: The choroid is responsible for supplying blood to the outer retina and RPE. Aerobic exercise improves overall vascular reactivity and endothelial function, which helps maintain adequate choroidal perfusion. This enhanced blood flow is vital for delivering essential nutrients and removing waste from the RPE, translating systemic cardiovascular improvements directly into better ocular perfusion pressure and health.
What are the biggest barriers to activity for AMD patients?
The primary barriers to physical activity for patients with Age-Related Macular Degeneration (AMD) stem from the direct consequences of vision loss, rather than the systemic nature of the disease draining their energy. These barriers break down into two main categories:
- Physical Navigation Challenges: The loss of vision inherently causes difficulties with balance, navigation, and hazard detection. Because AMD diminishes contrast sensitivity, depth perception, and visual field integrity, patients face an actual fall risk that is 2 to 8 times higher than that of their visually normal peers
- The Fear of Falling (FoF): Identified as the most significant non-physiological barrier, this psychological phenomenon drives a "vicious cycle" of decline. Recognizing their increased risk of falling, patients develop a pervasive fear and intentionally restrict their movement, daily activities, and travel outside the home to protect themselves.
- Unfortunately, this maladaptive coping mechanism leads to physical deconditioning, including muscle atrophy, reduced proprioception, and poorer balance. Paradoxically, this deconditioning actually increases their risk of falling, which only reinforces their fear and perpetuates a continuous cycle of inactivity and functional decline.
What exercise protocols are recommended to help prevent vision loss?
To effectively protect against vision loss and overcome the unique barriers of visual impairment, the sources recommend a combination of specific exercise dosing and structured, comprehensive interventions.
Exercise Type and Dosing Recommendations
- Prioritize Moderate-to-Vigorous Physical Activity (MVPA): Engaging in MVPA, such as brisk walking or running, is strongly recommended because it demonstrates the most robust causal link to reducing the risk of Age-Related Macular Degeneration (AMD).
- Aim for >150 minutes per week: The clinical target is to achieve more than 150 minutes of moderate activity weekly, which ideally translates to walking or running 2 to 4 kilometers per day. Risk reduction is incremental, and even moving from a sedentary lifestyle to just 2 km per day provides a significant 36% reduction in AMD incidence.
The Empowerment-Based Physical Activity Intervention (EPI) Model Because simply prescribing exercise is often ineffective for visually impaired patients experiencing a fear of falling, the sources highlight a specialized 6-month protocol known as the EPI model. This holistic approach includes:
- Targeted Balance Training: Patients engage in group classes twice a week for one hour, focusing specifically on strength, flexibility, and stability to directly mitigate actual fall risks.
- Adapted Sports: Activities such as adapted table tennis are utilized to safely promote hand-eye coordination, reaction time, and crucial social engagement
- Health Coaching: The protocol incorporates scheduled coaching sessions that use motivational interviewing to help patients build self-efficacy, reframe negative beliefs about their physical capabilities, and directly address their fear of falling.
- Community Integration: To ensure the exercise habits are sustainable long-term, the program deliberately transitions patients into municipal gyms or community sports where the staff have been educated on the specific needs of visually impaired clients.
Clinical Assessment and Environmental Support
- Objective Tracking: Because AMD patients frequently underestimate their inactivity, protocols should use accelerometers or validated wearable devices for baseline assessments rather than relying solely on self-reported questionnaires.
- Occupational Therapist (OT) Assessments: Exercise regimens should always be paired with home safety assessments led by OTs. By expertly identifying hazards and implementing modifications like better lighting or grab bars, OTs can successfully reduce fall occurrences and create a safer environment that encourages movement.
Can wearable devices improve exercise consistency for AMD patients?
The current research strongly recommend using them because they are critical for accurately tracking consistency and establishing an objective baseline for AMD patients.
Here is why wearable devices, such as accelerometers, are considered essential in clinical protocols for AMD patients:
- Overcoming the "Subjective Illusion": There is a significant disconnect between what AMD patients think they are doing and their actual activity levels. When relying on self-reported questionnaires, the significant activity deficit in the AMD population is often masked. However, objective measurements from accelerometers reveal the reality: healthy individuals actually engage in 33–34% more moderate-to-vigorous physical activity (MVPA) than patients with AMD.
- Identifying Activity Fragmentation: Wearable data helps clinicians spot "activity fragmentation." Instead of engaging in sustained movement, patients with visual field damage often only manage short, broken bursts of activity followed by rest. Tracking this fragmentation is crucial because it serves as an early marker of functional decline, poor physiological reserve, and higher fatigability.
- Creating Accurate Clinical Assessments: Because AMD patients frequently underestimate their inactivity, clinical guidelines explicitly advise against relying solely on self-reports. Utilizing validated wearable devices provides the objective data necessary to properly assess a patient's true mobility deficit and tailor interventions (like the EPI model) to their specific needs
How does physical activity help prevent macular degeneration?
Building on the biological mechanisms discussed earlier—such as reducing systemic inflammation, lowering oxidative stress, and improving choroidal perfusion—physical activity translates these physiological benefits into powerful, measurable prevention against the onset of Age-Related Macular Degeneration (AMD).
The evidence demonstrates how physical activity helps prevent AMD across several key areas:
- Establishing a Direct Causal Link: A major question in AMD research has been whether physical activity actually prevents AMD, or if people with early vision loss simply exercise less (reverse causality). Recent Mendelian randomization studies have resolved this by using genetic variants to confirm a direct causal relationship, showing that moderate-to-vigorous physical activity (MVPA) actively reduces the risk of developing AMD.
- Acting as a Primary Preventative Measure: Longitudinal studies, such as the E3 Consortium analysis of over 14,000 adults, reveal that physical activity is highly effective at preventing the initial onset of early AMD. However, once early AMD is established, physical activity does not appear to significantly halt the progression to late-stage AMD. This suggests a "metabolic rescue" hypothesis: exercise creates systemic conditions that prevent initial drusen accumulation, but once the disease cascade begins, local ocular pathology may take over, making exercise most effective when used as primary prevention.
- Providing a "Convex" Dose-Response Benefit: The National Runners’ Health Study established that the protective benefits of vigorous activity increase incrementally with volume, independent of cardiovascular fitness or body weight. Risk reductions are steepest when transitioning from a completely sedentary lifestyle to modest activity. Compared to those running less than 2 km per day:
- Running 2–4 km/day reduces AMD risk by 19%.
- Running >4 km/day reduces risk by 42% to 54%.
- Running ≥8 km/day reduces risk by 54% to 59%.
- Influencing Specific Demographics: The preventative effects of physical activity can be modified by age and gender. Some cohort studies indicate that the strongest protective effect against early AMD onset occurs around the sixth decade of life. Furthermore, studies like the Melbourne Collaborative Cohort Study have identified gender-dimorphic benefits, finding that frequent, vigorous exercise reduces the risk of intermediate AMD specifically in women by 22%, an association that was not observed in men.
Ultimately, engaging in regular physical activity prevents AMD by regulating systemic health risk factors before local retinal pathology can take hold, providing the most substantial protective benefits when implemented early and at moderate-to-vigorous intensities
What are the gender-specific benefits of vigorous exercise for women?
Frequent vigorous exercise provides a distinct, protective benefit against intermediate Age-Related Macular Degeneration (AMD) specifically for women. Women who engage in vigorous physical activity three or more times per week experience a 22% decrease in the odds of developing intermediate AMD. This significant risk reduction remains robust even after controlling for common AMD confounders and risk factors such as age, smoking, diet, and region of descent.
Crucially, this protective association between frequent vigorous exercise and reduced AMD risk is not found in men. This gender-specific benefit is not an isolated finding; other large-scale research, such as the Tromsø study, has similarly demonstrated a protective association against AMD for women but not for men.
Researchers hypothesize that this gender discrepancy might be partially explained by a "survival bias" rather than purely biological differences. Because men generally face a higher risk of mortality at younger ages compared to their female counterparts, the men who survive to participate in older-age assessments are often exceptionally healthy on average. This inherent healthiness lowers their baseline risk for developing AMD, which may statistically mask the specific benefits derived from exercise.
Why do women see more benefit from vigorous exercise?
While the exact reasons for this gender discrepancy remain speculative, researchers propose two primary hypotheses for why women appear to derive a more observable benefit from vigorous exercise regarding AMD prevention:
- Biological and Hormonal Differences: The female-specific protection may be rooted in biology. Researchers suggest that the metabolic changes induced by exercise might interact specifically with post-menopausal hormonal profiles. Additionally, there may be inherent differences in the baseline inflammatory status between aging men and women, meaning exercise could impact their respective inflammatory pathways differently.
- Survival Bias: As noted previously, a statistical phenomenon known as "survival bias" may mask the benefits of exercise for men. Because men generally face a higher risk of mortality at younger ages compared to women, the men who survive long enough to participate in these older-age cohort studies tend to be exceptionally healthy on average. These surviving men already have a lower baseline risk of developing AMD, which makes it statistically difficult to measure the additional protective effects of physical activity that are clearly visible in the female participants.
How much does vigorous activity reduce intermediate AMD risk?
Frequent vigorous physical activity (engaged in three or more times per week) reduces the odds of developing intermediate AMD by 22% in women.
Crucially, this protective benefit is highly gender-specific. For men, engaging in the exact same frequency of vigorous exercise does not yield any significant risk reduction for intermediate AMD
Does sunlight exposure during outdoor activity increase AMD risk?
The current evidence does not strongly support the idea that sunlight exposure during outdoor physical activity increases the risk of Age-Related Macular Degeneration (AMD). While a 2012 meta-analysis suggested that increased sunlight exposure could heighten AMD risk, researchers caution that this conclusion was skewed by several small studies relying on unadjusted estimates. As a result, experts maintain that much stronger evidence is needed to prove that sunlight exposure negatively confounds the established benefits of physical activity.
When evaluating the specific impacts of indoor versus outdoor exercise, researchers have found no clear indication that sunlight exposure diminishes the protective effects of being active. In fact, evidence points to several potential advantages of outdoor activity:
- No increased risk from outdoor time: The Eye Disease Case-Control Study Group analyzed lifestyle habits and reported that outdoor leisure time, working outdoors, and wearing sunglasses were not associated with the prevalence of AMD.
- Outdoor activities show specific protective benefits: The Beaver Dam Eye Study found that the number of blocks walked (an outdoor activity) was associated with a decreased incidence of exudative (wet) AMD, whereas the number of stair flights climbed (an indoor activity) did not demonstrate the same protective association.
- Potential Vitamin D benefits: Researchers hypothesize that walking outdoors may provide additional protection against AMD because it is highly correlated with increased blood vitamin D levels, which may beneficially mediate the disease's progression.
Ultimately, the protective physiological benefits of engaging in physical activity against AMD appear to remain robust regardless of whether that activity takes place indoors or outdoors
What is the metabolic rescue hypothesis in AMD prevention?
The "metabolic rescue" hypothesis proposes that physical activity is most effective as a primary preventative measure to stop the initial onset of Age-Related Macular Degeneration (AMD), rather than as a treatment to halt progression once the disease is already established.
According to this hypothesis, the process works in two distinct phases:
- Before AMD Onset (The "Rescue"): In a healthy retina, the systemic benefits generated by exercise—such as improved lipid profiles, enhanced blood perfusion, and reduced oxidative stress—are sufficient to maintain the homeostasis of the retinal pigment epithelium (RPE). These systemic improvements effectively "rescue" the tissue from metabolic strain and prevent the initial formation and accumulation of drusen.
- After Early AMD is Established: Once the pathological cascade begins, the disease becomes increasingly driven by localized ocular mechanisms, such as complement activation, local oxidative stress, and RPE senescence. These local ocular issues are much less responsive to the systemic benefits of exercise, which explains why physical activity is highly effective at preventing the transition from "no AMD" to "early AMD," but does not significantly halt the progression from early to late-stage AMD.
References:
- Zhou-et-al-2025-genetically-determined-physical-activity-levels-sedentary-behaviours-and-their-association-with-the.pdf
- The Impact of Physical Exercise on Oxidative and Nitrosative Stress: Balancing the Benefits and Risks - MDPI, accessed January 18, 2026, https://www.mdpi.com/2076-3921/13/5/573
- Oxidative stress: role of physical exercise and antioxidant nutraceuticals in adulthood and aging - PMC - PubMed Central, accessed January 18, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC5908316/
- Reductive carboxylation is a major metabolic pathway in the retinal pigment epithelium | PNAS, accessed January 18, 2026, https://www.pnas.org/doi/10.1073/pnas.1604572113
- Aerobic Exercise Protects Retinal Function and Structure from Light-Induced Retinal Degeneration - PMC - NIH, accessed January 18, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC3921416/
- Aerobic Exercise Protects Retinal Function and Structure from Light-Induced Retinal Degeneration | Journal of Neuroscience, accessed January 18, 2026, https://www.jneurosci.org/content/34/7/2406.short
- Enhancing Retinal Resilience: The Neuroprotective Promise of BDNF in Diabetic Retinopathy - MDPI, accessed January 18, 2026, https://www.mdpi.com/2075-1729/15/2/263
- Effect of isometric exercise on choroidal blood flow in patients with age-related macular degeneration - PubMed, accessed January 18, 2026, https://pubmed.ncbi.nlm.nih.gov/20837789/
- EFFECT OF ISOMETRIC EXERCISE ON CHOROIDAL BLOOD FLOW IN PATIENTS WITH AGE-RELATED MACULAR DEGENERATION (AMD) - PubMed Central, accessed January 18, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC4077432/
- Exercise for Eyes and Vision - American Academy of Ophthalmology, accessed January 18, 2026, https://www.aao.org/eye-health/glasses-contacts/exercise-eyes-vision-4
- Age-Related Macular Degeneration Is Associated with Less Physical Activity among US Adults: Cross-Sectional Study | PLOS One - Research journals, accessed January 18, 2026, https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0125394
{kind=link}
Leave a comment
This site is protected by hCaptcha and the hCaptcha Privacy Policy and Terms of Service apply.