Systemic Metabolomics and the Pathological Trias of Age-Related Macular Degeneration: Advanced Biomarker Stratification and Therapeutic Modulation Beyond AREDS2
Introduction: The Eye as a Systemic Metabolic Outpost
Age-related macular degeneration (AMD) is a highly prevalent, progressive retinal disorder and a primary driver of irreversible central vision loss in individuals over fifty years of age. Epidemiological modeling indicates that the global burden of AMD is escalating rapidly. While some conservative analyses placed the number of diagnosed individuals at approximately 10 million in 2020 with projections to double by 2040 , broader population studies estimate that approximately 196 million individuals were affected in 2020, a figure projected to rise to 288 million by 2040. For decades, the standard clinical protocol for slowing the progression of non-exudative (dry) AMD has remained relatively static, focusing almost exclusively on localized, defensive strategies. These include recommending smoking cessation, promoting a Mediterranean diet, and prescribing over-the-counter antioxidant mineral supplements modeled on the Age-Related Eye Disease Study 2 (AREDS2) formulation.
Although this defensive regimen has successfully delayed progression for many patients with intermediate disease, it is conceptually limited by treating the eye as an isolated metabolic system. Emerging clinical science demonstrates that AMD is not merely a localized ocular failure, but rather the phenotypic expression of a complex, systemic metabolic crisis. This paradigm shift has been accelerated by the EYE-RISK Project, a multi-center consortium that analyzed 5,923 individuals across five major European cohorts, including the Rotterdam Study, ALIENOR, EUGENDA, MARS, and CORRBI. Utilizing a high-throughput proton nuclear magnetic resonance (NMR) spectroscopy platform to profile 146 circulating blood metabolites, researchers evaluated the relationships between systemic metabolic alterations and the development and progression of AMD.
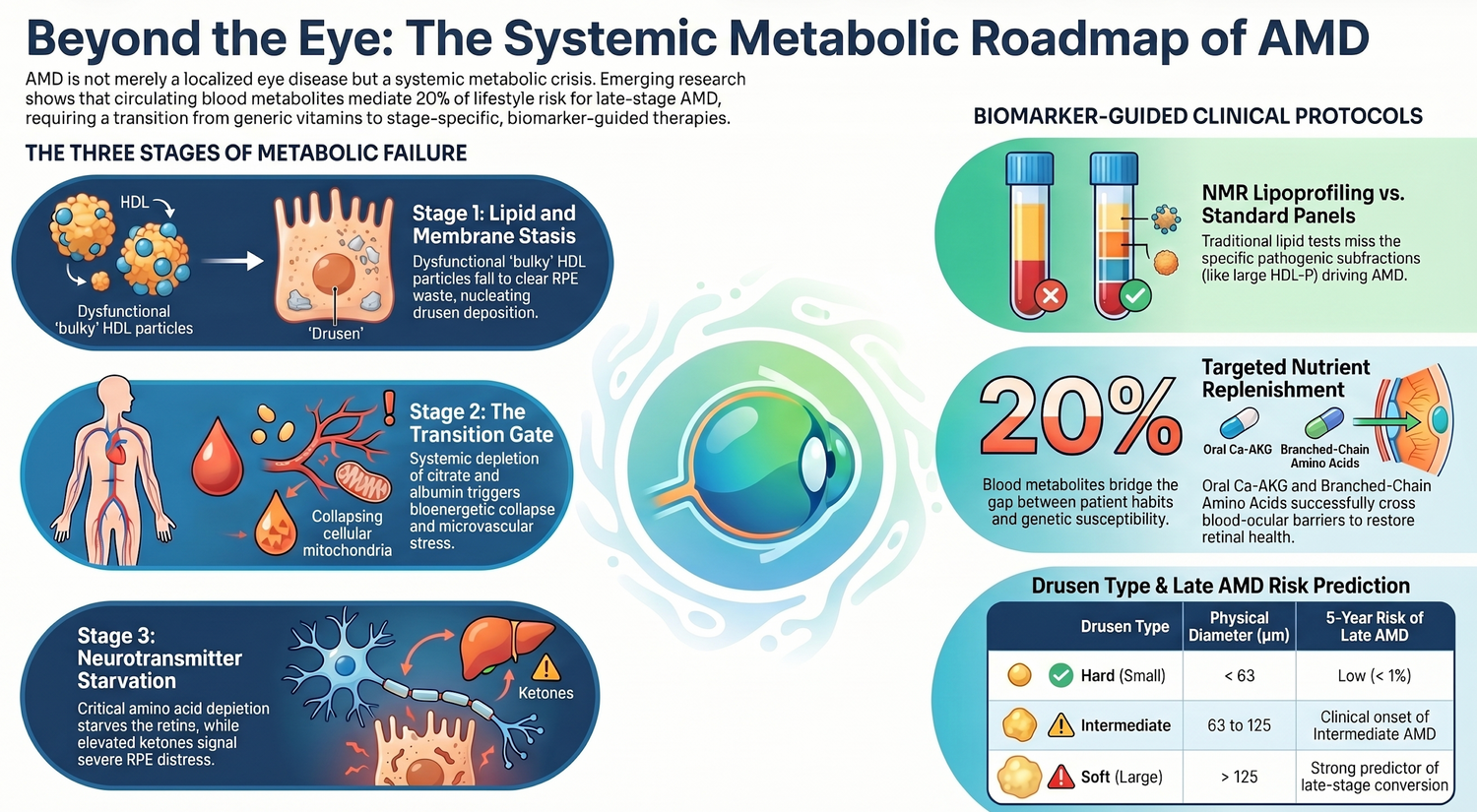
 The EYE-RISK Project constructed a comprehensive tripartite framework incorporating a Genetic Risk Score (GRS), a Lifestyle Risk Score (LRS), and a Metabolite Risk Score (MRS). A critical finding of this study is that the circulating blood metabolome (MRS) mediates approximately $5\%$ of the total genetic risk (GRS) and a substantial $20\%$ of the entire impact of lifestyle factors (LRS) on late-stage AMD conversion. Consequently, circulating metabolites represent a dynamic, modifiable physiological interface that bridges genetic susceptibility and lifestyle choices.Characterizing these systemic metabolic shifts across distinct stages of AMD pathobiology allows clinical practitioners to transition from passive, empirical supplementation to highly targeted, biomarker-guided metabolic interventions.
The EYE-RISK Project constructed a comprehensive tripartite framework incorporating a Genetic Risk Score (GRS), a Lifestyle Risk Score (LRS), and a Metabolite Risk Score (MRS). A critical finding of this study is that the circulating blood metabolome (MRS) mediates approximately $5\%$ of the total genetic risk (GRS) and a substantial $20\%$ of the entire impact of lifestyle factors (LRS) on late-stage AMD conversion. Consequently, circulating metabolites represent a dynamic, modifiable physiological interface that bridges genetic susceptibility and lifestyle choices.Characterizing these systemic metabolic shifts across distinct stages of AMD pathobiology allows clinical practitioners to transition from passive, empirical supplementation to highly targeted, biomarker-guided metabolic interventions.
Stage 1: The Lipid and Membrane Stasis Stage (Early-to-Intermediate AMD)
Systemic Dyslipidemia and the Dysfunctional HDL Paradox
In the early and intermediate stages of AMD, systemic metabolic dysregulation is almost exclusively driven by alterations in circulating lipids. The EYE-RISK metabolomic profiling revealed that $94\%$ of all significant circulating metabolite perturbations in early-to-intermediate AMD are lipid-related. Clinically, patients at this stage exhibit marked structural drops in all sizes of very-low-density lipoprotein (VLDL) subparticles, total serum triglycerides, and total cholesterol within VLDL. Concurrently, there is a significant systemic elevation in large to extra-large high-density lipoprotein (HDL) subparticles, as well as their primary structural protein, Apolipoprotein A1 (ApoA1). Logistic regression models demonstrate that total cholesterol in HDL/HDL2 is positively associated with early-to-intermediate AMD, yielding an odds ratio ($OR$) of $1.2$ ($p\text{-value}_{\text{FDR}} < 7.6 \times 10^{-5}$), while ApoA1 yields an $OR = 1.2$ ($p\text{-value}_{\text{FDR}} < 1.3 \times 10^{-3}$).

This lipid profile highlights a major physiological paradox. In cardiovascular disease, elevated HDL and ApoA1 are considered cardioprotective, yet in AMD, large-scale Mendelian randomization studies and observational cohorts confirm that elevated systemic HDL is causally linked to an increased risk of early and advanced AMD, as well as accelerated drusen deposition. This paradox is explained by the metabolic requirements of the outer retina. The retinal pigment epithelium (RPE) must continuously clear vast amounts of unesterified cholesterol and lipids derived from the daily phagocytosis of photoreceptor outer segment tips. To prevent toxic intracellular lipid pooling, the RPE relies on reverse cholesterol transport pathways to efflux these lipids across Bruch's membrane into the choriocapillaris, a process mediated by ATP-binding cassette transporters and systemic HDL acceptors. An elevation in circulating large and extra-large HDL subparticles, which represent lipid-satiated, structurally bulky carriers, indicates a systemic impairment of this cholesterol efflux capacity (CEC). Rather than facilitating clearance, these massive, inefficient HDL subparticles contribute to lipid stasis at the choriocapillaris-Bruch's membrane interface.
Drusen Genesis and the Liquid-Liquid Phase Separation Hypothesis
The extracellular deposits known as drusen, which accumulate between the basal lamina of the RPE and the inner collagenous layer of Bruch's membrane, are the hallmark pathognomonic feature of early-to-intermediate AMD. Drusen are highly heterogeneous but fundamentally rich in lipids and proteins, with lipids constituting up to $40\%$ of their total volume. Biochemical investigations into the molecular composition of human drusen support the "Meet, Greet, and Stick" hypothesis of drusenogenesis. Comprehensive "drusenomics" studies demonstrate that approximately $61\%$ of the identified proteins within human drusen uniquely originate from the systemic circulation, whereas only a minor fraction ($\sim 9\%$) is uniquely derived from local RPE or photoreceptor synthesis. These blood-derived lipids and proteins filter out of aging, increasingly resistive choroidal vessels and accumulate within Bruch's membrane.

The physical nucleation and growth of these deposits are driven by specific biochemical interactions. Drusen bodies are composed of cholesterol-containing lipid droplets forming a core structure upon which hydroxyapatite (HAP) spherules precipitate. The physical assembly of these components is heavily influenced by localized liquid-liquid phase separation (LLPS) of lipid-transport proteins. The RPE is the primary biosynthetic source of Apolipoprotein E (ApoE) in the retina. In individuals expressing the high-risk ApoE2 isoform, inefficient intracellular cholesterol transport leads to an accumulation of ceramides within the RPE, resulting in autophagic dysfunction and complement-mediated mitochondrial damage. Under this localized oxidative stress, reactive cysteines at positions 112 and 158 of the ApoE2 protein undergo thiol oxidation, triggering LLPS and the formation of biomolecular condensates. These condensates act as physical templates that trap circulating blood-derived lipids, apolipoproteins, and immunologic effectors. In contrast, the protective ApoE4 isoform lacks these reactive cysteines, rendering it resistant to phase separation and protecting the sub-RPE space from lipid-protein deposition.
Drusen size and morphology are highly predictive of clinical progression. The classification of these sub-RPE deposits is standardized based on their physical diameter and borders, as summarized in the table below:
|
Drusen Type |
Physical Diameter (μm) |
Borders and Morphology |
Prognostic Significance and AMD Association |
|
Hard Drusen (Small) |
$< 63$ |
Round, well-defined, distinct |
Considered normal age-associated findings; carry a low ($< 1\%$) five-year risk of progression to late AMD. |
|
Intermediate Drusen |
$63$ to $125$ |
Semisolid, moderately defined |
Represent a hybrid transitional form; clinically mark the onset of intermediate AMD when presenting in high numbers. |
|
Soft Drusen (Large) |
$> 125$ |
Large, poorly-defined, soft, mound-like |
Significantly impede the exchange of nutrients and waste; strongly predict progression to geographic atrophy or choroidal neovascularization. |
|
Cuticular Drusen |
$25$ to $75$ |
Extremely small, numerous, dot-like |
Tend to rapidly aggregate and coalesce into larger, soft deposits; carry a high prognostic risk for late AMD conversion. |

Genetic-Metabolomic Interactions and Mendelian Randomization Findings
The systemic lipid abnormalities identified in early-to-intermediate AMD do not occur in a genetic vacuum; they interact directly with host susceptibility loci. Genetic variants involved in lipid homeostasis—such as cholesteryl ester transfer protein (CETP), hepatic lipase C (LIPC), and ATP-binding cassette transporter A1 (ABCA1)—confer significant risk for AMD. For instance, the missense mutation D442G in the CETP gene, which is prevalent in East Asian populations, and the CETP risk variant $rs17231506$, both impair the transfer of cholesteryl esters from HDL to LDL, leading to elevated systemic HDL-C and a corresponding increase in neovascular AMD (nAMD) risk.Conversely, lipase C risk variants ($rs2043085$ and $rs2070895$) exhibit complex, opposite associations with circulating lipid levels, highlighting the molecular heterogeneity of the disease.

Furthermore, the relationship between circulating lipid-related metabolites and AMD is modulated by the complement system (CS). There is a synergistic interplay between systemic dyslipidemia and complement activation at the level of the RPE-choroid complex. The interactions between specific complement single nucleotide polymorphisms (SNPs) and blood lipid metabolites are structured as follows:
|
Genetic Variant (SNP) |
Associated Complement Pathway |
Circulating Lipid Metabolite Interaction |
Clinical Outcome & Interactive Effect |
|
CFH rs10922109 |
Complement Factor H |
Large & extra-large HDL subparticles |
Promotes the conversion of systemic HDL from an anti-inflammatory to a dysfunctional, pro-inflammatory carrier rich in complement proteins. |
|
C3 rs2230199 |
Complement Component 3 |
Total Cholesterol in $\text{HDL}_2$ |
In carriers without the risk allele, higher $\text{HDL}_2$is associated with increased AMD risk ($OR = 1.20$, $p\text{-value} = 0.005$); this association is inverted in carriers of the risk allele. |
|
rs116503776 |
Alternative Pathway Regulator |
Total Serum Triglycerides (TG) |
In carriers without the risk allele, higher triglycerides are protective ($OR = 0.84$, $p\text{-value} = 0.005$); in carriers with two risk alleles, higher TG significantly increases AMD risk ($OR = 2.3$). |

To establish causality among these complex lipid associations, phenome-wide Mendelian randomization (MR) studies have been conducted. Utilizing Mendelian randomization Bayesian model averaging (MR-BMA) to control for pleiotropy, researchers identified a dominant, causal role for serum sphingomyelin in the development of early AMD, yielding a marginal inclusion probability (MIP) of $0.76$ and a model-averaged causal estimate (MACE) of $0.29$.Sphingomyelin is a key component of cell membranes and circulating lipoproteins, and its accumulation is directly linked to the formation of pro-inflammatory sphingolipid derivatives at the outer blood-retinal barrier. Additionally, univariable MR analysis has supported causal roles for several systemic proteins, including S100-A5 ($OR = 1.07$, $p\text{-value} = 6.80 \times 10^{-6}$), cathepsin F ($OR = 1.10$, $p\text{-value} = 7.16 \times 10^{-5}$), and serine palmitoyltransferase 2 ($OR = 0.86$, $p\text{-value} = 1.00 \times 10^{-3}$), which regulates the rate-limiting step of sphingolipid de novo synthesis.

Clinical Monitoring: Advanced NMR Lipoprofiling
Because standard, routine lipid panels only measure generic, total concentrations of HDL-C and LDL-C, they lack the resolution to identify the specific pathogenic subfractions driving sub-RPE stasis. Clinicians managing patients at risk for AMD should request an Advanced NMR Lipoprofile. This diagnostic test utilizes proton NMR spectroscopy to directly quantify lipoprotein particle numbers, sizes, and diameters, including LDL particle number (LDL-P), VLDL size distribution, total serum triglycerides, and ApoA1 levels. Direct measurement of lipoprotein particle numbers by NMR is recognized by joint clinical consensus statements as a superior predictor of vascular disease risk compared to standard cholesterol concentration measurements, a principle that translates directly to the microvascular perfusion of the choriocapillaris.

Stage 2: The Transition Gate (Progression Dynamics)
Citrate, Albumin, and the Disruption of the Retinal Metabolic Shuttle
The progression from a stable, intermediate AMD phenotype to advanced geographic atrophy (GA) or choroidal neovascularization (CNV) represents a critical energetic and structural transition. Longitudinal metabolomic tracking from the EYE-RISK cohort identified two non-lipid markers in blood that act as independent, direct predictors of physical disease conversion: citrate and plasma albumin. When these two parameters fall below standard physiological thresholds, they indicate a systemic bioenergetic collapse and microvascular stress that destabilizes the blood-retinal barrier.
Citrate is a key intermediate of the tricarboxylic acid (TCA) cycle within mitochondria. Systemic depletion of citrate (which was found to be significantly reduced in patients converting to late AMD, yielding an $OR = 0.8$, $p\text{-value}_{\text{FDR}} = 2.7 \times 10^{-3}$) indicates a metabolic shift toward glycolytic inefficiency. This is highly detrimental to the outer retina, which relies on a specialized metabolic partnership between the RPE and the neural retina. Photoreceptors exhibit a robust rate of aerobic glycolysis, converting approximately $80\%$ to $90\%$ of their glucose into lactate. This lactate is exported into the subretinal space, where the adjacent RPE imports it to fuel its own mitochondrial TCA cycle, thereby "sparing" glucose for transport to the photoreceptors. A drop in systemic citrate levels indicates a broader failure of this cellular respiration cascade, leading to localized energy deprivation in both the RPE and photoreceptors.
Plasma albumin is the primary fluid-balance and antioxidant transport protein in the circulation. Falling levels of plasma albumin are associated with subclinical vascular inflammation, systemic oxidative stress, and chronic nutritional gaps. Albumin is responsible for binding and neutralizing free radicals and lipid peroxides. When systemic albumin plummets, the choriocapillaris becomes highly susceptible to oxidative injury and microvascular dysfunction. This accelerates chronic local ischemia, driving RPE dedifferentiation and the upregulation of vascular endothelial growth factor (VEGF), which triggers the angiogenic transition into neovascular AMD.

Lifestyle Modulators and the Gut-Retina Axis
The transition biomarkers, citrate and albumin, are highly modifiable by environmental and lifestyle factors. Regression analyses within the EYE-RISK Project demonstrated that smoking is strongly associated with an unfavorable, pro-inflammatory metabolic signature, specifically correlating with a decrease in systemic citrate levels ($\beta = -0.09$, $p\text{-value}_{\text{FDR}} < 3.1 \times 10^{-6}$). Conversely, a favorable lifestyle, characterized by high vegetable and fruit consumption, is associated with the upregulation of 49 circulating metabolites, including elevated levels of large HDLs ($\beta = 0.16 - 0.20$), which support systemic antioxidant capacity.
Furthermore, preclinical and clinical studies have identified a gut-retina axis, wherein dietary patterns shape the intestinal microbiome, thereby altering circulating metabolites that protect against outer retinal degeneration. The consumption of a high-glycemic-index (HG) diet, which mimic Western dietary patterns, alters the gut microbiota and leads to the development of key dry AMD features, including RPE hypopigmentation, localized atrophy, lipofuscin accumulation, and photoreceptor loss. Conversely, lower-glycemia (LG) diets promote the growth of beneficial gut taxa that synthesize protective microbial co-metabolites, most notably serotonin and short-chain fatty acids (SCFAs), which circulate systemically to reduce retinal inflammation and preserve mitochondrial function.
Additionally, there is a strong connection between the gut microbiome, systemic immune activation, and genetic risk.Patients with advanced AMD who carry the high-risk Complement Factor H allele (CFH Y402H) exhibit a distinct enrichment of Gram-negative, lipopolysaccharide (LPS)-producing bacterial taxa (such as Negativicutes and Escherichia-Shigella) in their gut microbiome. High levels of circulating LPS sequester CFH away from the retina, preventing it from binding to heparan sulfate on Bruch's membrane. This leads to uncontrolled alternative complement pathway activation, the deposition of the membrane attack complex (C5b-9) in subretinal tissues, and accelerated RPE geographic atrophy. Furthermore, wet AMD patients demonstrate a distinct gut microbiome signature, characterized by a significant enrichment of Clostridia class bacteria (such as Anaerotruncus, Oscillibacter, Ruminococcus torques, and Eubacterium ventriosum) and a marked depletion of the beneficial, anti-inflammatory taxon Bacteroides eggerthii.

The Stanford Phase 0 Interventional Trial: Proving Systemic-to-Ocular Target Engagement
While epidemiologic data has long linked systemic metabolites with retinal health, establishing direct, in vivo target engagement within the human eye remained a major clinical challenge. This gap was addressed by a landmark, prospective, open-label, single-arm interventional trial conducted at Stanford University (ClinicalTrials.gov ID: NCT07269704). The trial recruited patients undergoing sequential bilateral cataract surgery to evaluate whether oral administration of a longevity-associated mitochondrial metabolite, calcium alpha-ketoglutarate (Ca-AKG), could measurably remodel metabolic pathways within the living human eye.
The experimental protocol and results of the Stanford Phase 0 trial are detailed below:
- Clinical Protocol: Participants undergoing sequential, bilateral cataract extraction served as their own controls. A baseline aqueous humor (AH) sample (~100 $\mu\text{L}$) was collected during the first-eye cataract surgery.Beginning seven days prior to the second-eye surgery, the patient was administered an oral dose of $2 \text{ g/day}$ of Ca-AKG, taken twice daily. Post-supplementation AH was collected during the second-eye surgery.The paired samples underwent targeted metabolomic profiling using hydrophilic interaction liquid chromatography coupled with mass spectrometry (LC-MS).
- Aqueous Humor Proteomic Profiling in GA: Concurrently, DNA-aptamer-based proteomics was performed on AH samples from patients with clinically confirmed non-exudative late AMD with geographic atrophy. This analysis identified a coordinated depletion of 64 mitochondrial proteins in GA eyes, particularly enzymes regulating TCA cycle entry and flux, such as pyruvate dehydrogenase E1 subunit beta (PDHB) and dihydrolipoamide S-succinyltransferase (DLST), confirming a localized, intraocular state of oxidative bioenergetic failure.
- Trial Outcomes: Following oral Ca-AKG supplementation, metabolomic analysis of the post-supplementation AH revealed a significant increase in intraocular $\alpha\text{-ketoglutarate}$ levels and a marked rise in the intraocular $\alpha\text{-KG-to-succinate}$ ratio ($p\text{-value} < 0.05$). This was accompanied by coordinated, downstream shifts across multiple TCA intermediates, consistent with enhanced mitochondrial TCA cycle flux and improved ATP production capacity.
- Clinical Significance: This trial provided the first in-human, in vivo proof of concept that a systemic, orally administered metabolic therapy can successfully cross the blood-ocular barriers, engage intraocular metabolic targets, and physically remodel the bioenergetic pathways of the living human eye, paving the way for biomarker-guided metabolic trials in AMD.
Stage 3: Late AMD (The Amino Acid and Ketone Crisis)
Essential Amino Acid Depletion and Retinal Neurotransmitter Starvation
Once AMD progresses to its advanced, vision-threatening late stages—either non-exudative geographic atrophy or exudative choroidal neovascularization—the systemic metabolome enters a state of severe, chronic metabolic stress.The EYE-RISK Project identified a highly significant depletion of essential and aromatic amino acids in late AMD patients, specifically valine, leucine, histidine, phenylalanine, and tyrosine ($OR = 0.6 - 0.8$, $p\text{-value}_{\text{FDR}} < 1.5 \times 10^{-3}$).
Because branched-chain amino acids (BCAAs) such as valine and leucine are essential, the body cannot manufacture them, and their systemic levels are entirely dependent on dietary intake, metabolic clearance, and transport efficiency.Systemic depletion of these essential amino acids directly starves the retina of the raw precursors required for local neurotransmission and cellular repair. While the neural retina lacks a direct, systemic blood supply, it is highly metabolically coupled with the adjacent RPE. Tracing studies utilizing $^{15}\text{N}$-labeled proline demonstrate that the RPE acts as a metabolic manufacturing hub, expressing proline dehydrogenase (PRODH) to assimilate nitrogen and synthesize and export 13 amino acids—most notably glutamate, aspartate, glutamine, alanine, and serine—directly to the neural retina.
Under physiological conditions, the transamination of the BCAAs valine and leucine with $\alpha\text{-ketoglutarate}$via branched-chain aminotransferases (BCAT) isozymes is a primary mechanism for the de novo synthesis of glutamate in extrahepatic tissues. Glutamate is the dominant excitatory neurotransmitter in the central nervous system and the retina, responsible for transferring visual signals from photoreceptors to second-order bipolar neurons. When circulating levels of valine and leucine run low, this localized transamination is severely compromised, disrupting the glutamate/glutamine cycle and impairing de novo synthesis of glutamate. This leads to synaptic dysfunction, neurotransmission failure, and accelerated outer retinal degeneration.

Notably, the role of BCAAs in the retina exhibits a complex biological duality. In chronic metabolic disorders such as diabetic retinopathy, pathologically elevated levels of systemic BCAAs accumulate in retinal Müller glia, where they undergo excessive transamination to produce neurotoxic levels of glutamate, leading to excitotoxicity and retinal ganglion cell death. Conversely, in degenerative retinal diseases such as retinitis pigmentosa and glaucoma, targeted BCAA supplementation plays a neuroprotective role, preventing photoreceptor and ganglion cell death by activating the mTOR pathway, promoting mitochondrial ATP synthesis, and restoring ionic homeostasis in ischemic regions.
Ketogenic Spikes as a Marker of Outer-Retinal Distress
In stark contrast to the depletion of amino acids, late-stage AMD is characterized by a massive, highly significant elevation in the circulating ketone bodies acetoacetate and 3-hydroxybutyrate ($\beta\text{-HB}$), yielding an $OR = 1.4$ ($p\text{-value}_{\text{FDR}} < 2.5 \times 10^{-8}$). While ketogenesis occurs primarily in the liver, the RPE is an active ketogenic tissue, expressing high levels of the rate-limiting enzyme 3-hydroxy-3-methylglutaryl-CoA synthase 2 (HMGCS2) and $\beta\text{-hydroxybutyrate}$ dehydrogenase 1 (BDH1).
Under physiological conditions, the RPE utilizes mitochondrial $\beta\text{-oxidation}$ of fatty acids derived from circulating lipoproteins and the phagocytosis of photoreceptor outer segments to generate acetyl-CoA, which is subsequently converted into acetoacetate and $\beta\text{-HB}$. Monocarboxylate transporters (MCT1 and MCT7) then export these ketone bodies across both the apical and basolateral RPE membranes. The adjacent photoreceptors and Müller glia actively uptake these ketone bodies to fuel their own mitochondrial respiration, utilizing them as alternative energy substrates to preserve precious glucose. Additionally, extracellular $\beta\text{-HB}$ acts as a potent signaling molecule, activating the hydroxycarboxylic acid receptor 2 (HCAR2/GPR109A) and the Nrf2 transcription factor to induce antioxidant enzymes (such as HO-1 and NQO1), thereby maintaining blood-retinal barrier integrity and suppressing neuroinflammation.
However, under the severe oxidative stress and lysosomal degradation failure characteristic of late AMD, the RPE clearance machinery is overwhelmed. In disease models with defects in phagosome maturation (such as the Abca4knockout model), the RPE is unable to process the daily load of lipid-rich outer segment disks, leading to the toxic accumulation of lipofuscin and lipid debris in the sub-RPE space. To cope with this severe lipotoxicity and preserve mitochondrial function, the RPE significantly upregulates fatty acid oxidation and ketogenesis. Thus, the marked systemic elevation of acetoacetate and 3-hydroxybutyrate observed in late-stage AMD serves as a systemic biomarker for localized outer-retinal distress and RPE-specific lipotoxicity.
Clinical Application: Targeted Amino Acid and Ketone Modulation
To counter the systemic amino acid drain and local lipid stress of late-stage AMD, clinicians must implement target-formulated amino acid replenishment strategies and metabolic stabilizing therapies. Routine diagnostic monitoring should include a fasting Plasma Amino Acids Profile alongside a quantitative Serum Ketone Panel, utilizing high-sensitivity mass spectrometry (LC-MS) rather than commercial enzymatic kits, which are prone to artifact and lack the sensitivity to accurately measure physiological ketone variations.
Targeted replenishment of the essential BCAA pool via oral supplementation of pure valine and leucine can bypass systemic depletion, providing the nitrogen donors required to sustain retinal glutamate signaling and activate cytoprotective mTOR pathways. Furthermore, preclinical and clinical data have validated the efficacy of specific, phase-targeted amino acid therapies in managing degenerative retinal and macular diseases.
The therapeutic evidence, physiological mechanisms, and recommended clinical dosages for targeted amino acid modulation are structured in the table below:
|
Amino Acid / Peptide |
Physiological Target & Mechanism of Action |
Preclinical & Clinical Evidence |
Recommended Clinical Dosage & Protocol |
|
Taurine |
Mitigates photochemical stress; upregulates glutathione, SOD, and catalase; inhibits apoptotic cascades; restores RPE phagocytosis. |
Preserved photoreceptor outer segments and ERG responses in dystrophic RCS rats and glaucoma models. |
• Oral: $0.2 \text{ M}$ in drinking water or $1.2\% - 4\%$dietary loading. • Intravitreal: $320 \text{ nM}$ or $2\ \mu\text{L}$ dose. |
|
Histidine |
Serves as a proton buffer; chelates metal ions; scavenges ROS; inhibits the stabilization of hypoxia-induced HIF-1$\alpha$. |
Dramatically reduced pathologic retinal neovascularization in oxygen-induced retinopathy (OIR) models. |
• Oral: $5000\text{ mg/kg}$ body weight. |
|
Serine |
Rescues mitochondrial structure; activates cytoprotective AMPK and mTOR; balances glutathione; prevents deoxysphingolipid synthesis. |
Currently in Phase 2a clinical trial (NCT04907084) for MacTel; shown to dramatically reduce neurotoxic lipid levels. |
• Oral: Up to $400\text{ mg/kg/day}$ (well-tolerated and safe in humans). |
|
Glutamine |
Supports de novo NADPH generation in rod photoreceptors; protects the retina from oxidative stress-induced apoptosis. |
Promoted by dietary antioxidants and omega-3 long-chain PUFAs to upregulate glutamine synthesis in Müller glia. |
• Dietary Synergists:Co-administered with high-purity Lutein, Zeaxanthin, and Lycopene. |
|
Arginyl-Glutamine |
Inhibits retinal neovascularization by directly downregulating ocular Vegf mRNA expression. |
Demonstrated robust anti-angiogenic efficacy in hyperoxic retinopathy models. |
• Experimental:Target-formulated dipeptide blend. |
|
L-Isoleucine |
Physiologically regulates retinal vessel development; delays early-stage vascular overgrowth under hyperglycemic stress. |
Successfully normalized vascular growth in Phase I retinopathy of prematurity models. |
• Systemic:Administered as part of a targeted, clinical-grade BCAA formulation. |

Conclusions and Actionable Clinical Practice Protocols
Systemic clinical science, established by the EYE-RISK consortium and supported by targeted interventional trials, has demonstrated that age-related macular degeneration is a localized manifestation of a chronic, systemic metabolic crisis.Because circulating blood metabolites mediate $20\%$ of the entire impact of lifestyle factors on late-stage AMD conversion, relying on empirical, non-specific nutritional advice is insufficient for optimal patient care. By mapping specific systemic metabolomic alterations, clinical practitioners can move past generic vitamin formulas to implement a personalized, data-driven shield for the eyes.

To integrate these findings into clinical practice, the following stage-specific protocols should be utilized:
Stage 1: The Lipid and Membrane Stasis Protocol (Early-to-Intermediate AMD)
- What to Measure: Order an Advanced NMR Lipoprofile to measure VLDL subparticle sizes, total VLDL particle number, large and extra-large HDL particle numbers (HDL-P), total serum triglycerides, and the ApoB to ApoA1 ratio. Conventional lipid panels are inadequate for identifying these subfractions.
- Pathological Rationale: High concentrations of bulky, lipid-satiated large and extra-large HDL subparticles indicate a systemic failure of reverse cholesterol transport, preventing the clearance of RPE lipid waste. Under localized oxidative stress, this lipid stasis promotes the liquid-liquid phase separation of ApoE2, nucleating drusen deposition within Bruch's membrane.
- Therapeutic Modulation: Initiate high-dose, high-purity Omega-3 long-chain polyunsaturated fatty acids (maximizing EPA and DHA to expand the systemic Omega-3 Index) to reduce VLDL subparticles and enhance choriocapillaris membrane fluidity. Supplement with bioavailable, lipophilic antioxidants (such as Lutein, Zeaxanthin, and Lycopene) to shield circulating apolipoproteins from oxidative modifications, reducing their susceptibility to phase separation and Bruch's membrane deposition. Promote low-glycemia dietary patterns to enrich beneficial gut microbiota and increase protective circulating metabolites (such as serotonin and SCFAs), which mitigate localized retinal complement activation and drusen growth.
Stage 2: The Transition Gate Protocol (Progression Dynamics)
- What to Measure: Regularly assess Serum Citrate and Plasma Albumin levels as predictive metabolic markers of late-stage conversion. These markers must not be viewed as generic hepatic or renal metrics, but rather as key indices of outer blood-retinal barrier stability.
- Pathological Rationale: Depleted citrate represents a systemic bioenergetic collapse, disrupting the lactate-glucose metabolic shuttle between the RPE and photoreceptors. A drop in plasma albumin indicates a loss of blood antioxidant transport, driving microvascular ischemia, localized hypoxia, and the upregulation of angiogenic VEGF.
- Therapeutic Modulation: Stabilize fluid kinetics and support mitochondrial respiration by optimizing clean, highly bioavailable protein absorption to maintain plasma albumin levels within an optimal, anti-inflammatory range. Enhance mitochondrial TCA cycle efficiency by increasing organic vegetable and fruit consumption, which is clinically proven to boost systemic citrate levels. In patients exhibiting rapid progression or geographic atrophy, consider targeting anaplerotic pathways with oral Calcium Alpha-Ketoglutarate (Ca-AKG) supplementation ($2 \text{ g/day}$), which has been clinically demonstrated in humans to cross the blood-retinal barrier, increase intraocular $\alpha\text{-KG}$ levels, and enhance intraocular mitochondrial energy metabolism.
Stage 3: The Neuroprotective Replenishment Protocol (Late AMD)
- What to Measure: Obtain a comprehensive fasting Plasma Amino Acids Profile and a high-sensitivity, mass spectrometry-based Serum Ketone Panel, tracking acetoacetate and 3-hydroxybutyrate levels.
- Pathological Rationale: Severe systemic depletion of essential and aromatic amino acids (valine, leucine, phenylalanine, tyrosine, and histidine) starves the neural retina of the precursors required for de novo glutamate/glutamine synthesis, causing synaptic transmission failure. Concurrently, elevated acetoacetate and $\beta\text{-HB}$ serve as systemic indicators of lysosomal failure and RPE lipotoxicity.
- Therapeutic Modulation: Administer a targeted, clinical-grade amino acid replenishment formula rich in pure, essential branched-chain amino acids (Valine and Leucine) to bypass systemic depletion, support retinal glutamate synthesis, and activate cytoprotective mTOR pathways. Supplement with oral L-Serine ($400\text{ mg/kg/day}$) to reduce neurotoxic deoxysphingolipid levels and preserve photoreceptors, modeled on successful Phase 2a clinical protocols for MacTel type 2. Finally, integrate oral L-Histidine ($5000\text{ mg/kg}$) to prevent hypoxia-induced HIF-1$\alpha$ stabilization, and Taurine ($0.2\text{ M}$ in drinking water or $4\%$ dietary loading) to upregulate retinal antioxidant defense enzymes, preserve photoreceptor outer segments, and restore RPE lysosomal clearance capacity.

What are the three metabolic stages of macular degeneration progression?
Stage 1: The Lipid and Membrane Stasis Stage (Early-to-Intermediate AMD) This initial stage is almost exclusively driven by systemic dyslipidemia, with 94% of significant circulating metabolite perturbations being lipid-related. Patients typically experience a drop in very-low-density lipoprotein (VLDL) subparticles and serum triglycerides, while exhibiting a paradoxical systemic elevation in large to extra-large high-density lipoprotein (HDL) subparticles and Apolipoprotein A1 (ApoA1). While high HDL is normally cardioprotective, these large, bulky HDL carriers are inefficient in AMD, impairing the retinal pigment epithelium's (RPE) ability to clear cholesterol. This inefficiency causes lipid stasis and the nucleation of drusen (lipid and protein deposits) along Bruch's membrane.
Stage 2: The Transition Gate (Progression Dynamics) This stage marks the critical energetic and structural transition from intermediate AMD to advanced geographic atrophy or choroidal neovascularization. It is defined by the disruption of two critical non-lipid systemic biomarkers:
- Citrate Depletion: A drop in systemic citrate signals a systemic bioenergetic collapse. It indicates glycolytic inefficiency that deprives both the RPE and photoreceptors of localized energy.
- Plummeting Plasma Albumin: Albumin is a primary antioxidant and fluid-balance protein. A drop in its levels leaves the choriocapillaris highly susceptible to oxidative injury, microvascular dysfunction, and chronic local ischemia, which can trigger the expression of VEGF and promote neovascular (wet) AMD.
Stage 3: Late AMD (The Amino Acid and Ketone Crisis) In the advanced, vision-threatening stages of AMD, the systemic metabolome enters a state of severe chronic stress marked by two major metabolic shifts:
- Essential Amino Acid Depletion: There is a highly significant drop in circulating essential and aromatic amino acids, such as valine, leucine, histidine, phenylalanine, and tyrosine. Because the retina relies on these systemic precursors to synthesize neurotransmitters like glutamate, this depletion causes synaptic dysfunction, neurotransmission failure, and outer retinal degeneration.
- Ketogenic Spikes: Patients experience a massive elevation in circulating ketone bodies, specifically acetoacetate and 3-hydroxybutyrate. This occurs because the RPE's clearance machinery becomes overwhelmed by severe oxidative stress and toxic lipid accumulation. To survive this lipotoxicity and maintain mitochondrial function, the RPE upregulates fatty acid oxidation and ketogenesis, making these elevated ketone levels a systemic biomarker for outer-retinal distress
Can amino acid replenishment help slow late-stage AMD?
Evidence so far says: we don’t yet know that amino acid replenishment slows late‑stage AMD in humans, but multiple lines of data (including the paper you sent) suggest amino‑acid metabolism is important for retinal health and could become a therapeutic target, especially for photoreceptor/RPE support.
In late AMD, patients had:
- Lower systemic levels of essential/important amino acids: histidine, leucine, valine, tyrosine, phenylalanine, glutamine.
- Lower citrate and albumin (suggesting higher energy demand, subclinical under‑nutrition, or low muscle mass).
- Higher ketone bodies (3‑hydroxybutyrate, acetoacetate) and more inflammatory signal (glycoprotein acetyls) vs. earlier stages.
The authors interpret this as a systemic amino‑acid and energy‑metabolism disturbance linked to disease severity, not just a retinal issue. They explicitly note that low plasma histidine (in AMD) and similar patterns in other retinopathies suggest that supplementation with certain amino acids “may become a therapeutic measure and be of benefit to patients.”
So: amino‑acid depletion is clearly associated with late AMD, but association ≠ proof that giving back those amino acids slows progression.
What other data say about amino acids and the retina
Several independent strands (mostly preclinical or broad “retinopathy” data) support the biological plausibility of amino‑acid support:
- Glutamine and glutamate metabolism
- Preclinical work shows that glutamine processing is crucial for maintaining retinal thickness and photoreceptor survival; disrupting glutamine pathways leads to thinning and photoreceptor loss.
- A dietary supplement enriched in antioxidants and omega‑3 promoted in vivo increase of retinal glutamine and protected against light‑induced retinal degeneration in animals, suggesting that supporting glutamine synthesis is part of the protective effect.
- Proline as an RPE fuel
- Human RPE can use proline as a key nutrient and nitrogen source, generating other amino acids like glutamate, aspartate, glutamine, alanine, and serine.
- In a mouse AMD model, proline supplementation protected photoreceptors; AMD donor RPE cells showed impaired proline utilization.
- Amino acids in retinopathy in general (review)
- A systematic review of amino‑acid metabolism in DR, AMD, and ROP found that pathways involving alanine, aspartate, glutamate, glutamine, and leucine recur across retinal diseases.
- The authors highlight glutamine and arginine as promising biomarkers and suggest that decreased histidine in AMD plasma, without matching intraocular data, implies supplementation “may become a therapeutic measure.”
- BCAAs (leucine, valine, isoleucine)
- BCAA levels are altered across retinopathies; in some AMD/DR models they’re elevated and may drive ROS and excitotoxicity, but in other models BCAA supplementation protected retinal ganglion cells and photoreceptors via improved ATP production and mTOR activation.
- This duality means dosing and context are critical; “more BCAAs” is not automatically good.
In humans with AMD, we have good evidence for macular carotenoids and AREDS‑type antioxidants, but no completed RCT directly testing amino‑acid blends in late AMD yet.
So, could replenishment help slow late AMD?
Putting it together:
Biologically plausible? Yes.
- Late AMD shows systemic amino‑acid depletion and higher ketone bodies.
- Amino acids like glutamine, proline, histidine, and leucine clearly affect retinal metabolism and photoreceptor/RPE survival in models.
- Clinically proven in humans? Not yet.
- There are no large, late‑AMD trials showing that an amino‑acid supplement slows GA expansion or neovascular AMD progression. Existing positive human data in AMD are mostly carotenoids, vitamins, zinc, and omega‑3s.
- Risk profile?
- Modest correction of probable deficiencies (e.g., ensuring adequate essential amino acids and protein intake in older, sarcopenic AMD patients) is unlikely to be harmful and could have systemic benefits (muscle, immune, general resilience).
- High‑dose, single‑amino strategies (especially BCAAs) carry theoretical risks (e.g., altered glutamate excitotoxicity, increased ROS) and would need careful testing.
For a late‑AMD patient today:
- Do:
- Ensure adequate total protein intake and a balanced mix of essential amino acids via diet (and modest supplementation if intake is low).
- Optimize known, proven interventions: AREDS2‑type formulation, macular carotenoids, smoking cessation, Mediterranean‑style diet, blood pressure and cardiovascular risk control.
- Consider participation in clinical trials that are starting to probe metabolic interventions (e.g., proline, glutamine‑targeting supplements) when available.
- Be cautious with:
- High‑dose single amino acids (large BCAA loads, isolated glutamate, etc.) outside a study context.
- Any claim that “this amino‑acid powder will slow your late AMD”—the evidence simply isn’t there yet in humans.
For your formulation roadmap, amino‑acid replenishment looks like a research‑grade, mechanistically justified add‑on to established nutrient strategies, with the right positioning: “supports retinal metabolism and photoreceptor resilience” rather than “clinically proven to slow GA.”
A conservative, research‑grade amino‑acid concept for late AMD should: (1) correct likely age‑related and AMD‑associated deficits, (2) support retinal/RPE metabolism and glutathione, and (3) avoid high single‑AA loads or known smoker‑specific risks.
1. Design principles
Based on the metabolomics paper and broader retinal AA literature:
- Target pattern, not one molecule.
Late AMD is characterized by low histidine, leucine, valine, phenylalanine, tyrosine, glutamine and low citrate/albumin, with higher ketones and inflammation. A blend should address this pattern without overshooting any single AA. - Stay within “nutritional support” territory.
Use doses per amino acid well below those in disease‑specific high‑dose protocols (e.g., bodybuilding BCAA stacks, pharma‑grade glutamine dosing). - Support glutamate/glutamine and glutathione indirectly.
Focus on EAAs + glutamine + NAC/glycine rather than direct glutamate. - Avoid known risk zones.
- No mega‑dose BCAAs.
- No very high phenylalanine (PKU/rare metabolic disorders).
- No beta‑carotene co‑packaged for smokers.
2. Candidate amino acids and roles
Core “late‑AMD depleted” AA group
From the AMD metabolomics paper:
- Histidine
- Leucine
- Valine
- Tyrosine
- Phenylalanine
- Glutamine
These are essential or conditionally essential, and several play specific retinal roles:
- Histidine
- Essential, antioxidant properties, precursor of histamine.
- Depleted in AMD plasma; low levels also seen in other retinopathies.
- Candidate for modest supplementation to support antioxidant and buffering capacity.
- Leucine & Valine (BCAAs)
- Support protein synthesis, muscle mass, and serve as nitrogen donors for glutamate/glutamine, important in retinal neurotransmission.
- Need conservative dosing; excessive BCAA has been linked to metabolic issues and may worsen excitotoxicity in some contexts.
- Phenylalanine & Tyrosine
- Precursors for dopamine, norepinephrine, epinephrine; involved in retinal and central neurotransmission.
- Phenylalanine levels are low in late AMD, but very high phenylalanine is harmful in PKU and perhaps in severe systemic inflammation; keep modest.
- Glutamine
- Major fuel and nitrogen donor; key for glutamate cycle, glutathione synthesis, and RPE/photoreceptor support.
- Preclinical work suggests supporting glutamine pathways preserves retinal thickness and function.
Glutathione / redox support AA group (small doses)
- Glycine
- Substrate for glutathione; low glycine is common in aging; supports cytoprotective pathways.
- Cysteine (via N‑acetylcysteine, NAC)
- Rate‑limiting precursor for glutathione.
- NAC has a large safety record but can interact with nitrosative stress pathways; keep dose modest.
3. Tentative daily dose range (research‑grade, oral)
Assume an older adult (~60–85 years), 1–2 divided doses.
Per day, oral, total AA from the blend ~3–6 g (on top of diet), for use only in a supervised trial.
- Histidine: 250–500 mg/day
- Leucine: 500–1,000 mg/day
- Valine: 250–500 mg/day
- Phenylalanine: 150–300 mg/day
- Tyrosine: 150–300 mg/day
- Glutamine: 500–1,000 mg/day
- Glycine: 250–500 mg/day
- NAC (or cysteine equivalent): 150–300 mg/day
Total: roughly 2.2 – 3.4 g of AAs + 150–300 mg NAC, which is modest compared with standard EAA or BCAA supplements and well below clinical glutamine dosing used in ICU/GI settings.
4. Smoker‑safety and general risk considerations
Even though amino acids themselves do not carry the same smoker‑specific risks as beta‑carotene, your overall “metabolic” product must respect that population.
Key points:
- Phenylalanine
- Screen out individuals with known PKU or inborn errors of phenylalanine metabolism.
- Keep dose modest (≤300 mg/day) and monitor in early trials if you can measure plasma phenylalanine.
- BCAAs (leucine/valine)
- Avoid bodybuilding‑level doses; keep leucine ≤1 g/day and valine ≤500 mg/day, and monitor insulin sensitivity and liver markers in longer studies.
- NAC
- Generally safe at higher doses, but for older AMD patients with polypharmacy, keep 150–300 mg/day and monitor for GI upset, rare hypersensitivity.
- Co‑formulated ingredients
- Avoid beta‑carotene in smokers/former heavy smokers (separate from this AA blend, but critical if your eventual product line includes carotenoids).
- If combining with AREDS‑like formulations, adjust zinc and vitamin E to stay within known safe ranges and avoid additive risks.
- Renal function
- Older AMD patients often have some CKD. Any AA trial should exclude eGFR <30 and monitor creatinine/urea, especially if you move above the lower end of the dose ranges.
What role does citrate depletion play in AMD progression?
Citrate depletion acts as an independent, direct predictor of a patient's progression from stable, intermediate age-related macular degeneration (AMD) to advanced, vision-threatening stages like geographic atrophy or choroidal neovascularization. When systemic citrate falls below normal physiological thresholds, it signals a systemic bioenergetic collapse and a critical shift toward glycolytic inefficiency.
Because citrate is a key intermediate in the mitochondrial tricarboxylic acid (TCA) cycle, its depletion severely disrupts the specialized metabolic partnership between the retinal pigment epithelium (RPE) and the neural retina. Normally, photoreceptors rely on a high rate of aerobic glycolysis, converting glucose into lactate. This lactate is exported into the subretinal space and imported by the adjacent RPE to fuel its own mitochondrial TCA cycle, which allows the RPE to "spare" glucose for the photoreceptors.
A drop in systemic citrate indicates a broader failure of this cellular respiration cascade and the disruption of this lactate-glucose metabolic shuttle. This failure ultimately results in localized energy deprivation for both the RPE and the photoreceptors, driving the structural transition to late-stage AMD.
Longitudinal progression analyses confirm that lower levels of citrate are significantly associated with a higher cumulative risk of progressing from early-intermediate AMD to late AMD. Furthermore, citrate levels are highly sensitive to lifestyle choices; for example, smoking is strongly associated with a decrease in systemic citrate, whereas high vegetable and fruit consumption has been clinically proven to boost systemic citrate levels and support mitochondrial respiration
How do large HDL particles differ in AMD vs heart health?
While elevated levels of high-density lipoprotein (HDL) and its primary structural protein, Apolipoprotein A1 (ApoA1), are traditionally considered cardioprotective in cardiovascular disease, they present a major physiological paradox in age-related macular degeneration (AMD). Large-scale studies confirm that elevated systemic HDL is actually causally linked to an increased risk of both early and advanced AMD, as well as accelerated drusen (lipid deposit) formation.
The difference in how large HDL functions in AMD compared to heart health lies in the specific metabolic demands of the eye:
* Impaired Cholesterol Clearance: The retinal pigment epithelium (RPE) must constantly clear vast amounts of lipids and unesterified cholesterol generated from the daily recycling of photoreceptors. Normally, it relies on systemic HDL acceptors to transport these lipids away. However, elevated large and extra-large HDL subparticles act as lipid-satiated, structurally bulky carriers.
* Lipid Stasis and Drusen Formation: Because these massive HDL particles are already full, they indicate a systemic failure of reverse cholesterol transport. Rather than successfully clearing the RPE's lipid waste, these inefficient carriers contribute to lipid stasis at the interface of the choriocapillaris and Bruch's membrane, physically trapping lipids and promoting the nucleation of drusen deposits.
* Pro-inflammatory Shift: Furthermore, the genetic background of an AMD patient can alter the function of these particles. For example, the complement genetic variant CFH rs10922109 interacting with large HDL subparticles promotes the conversion of systemic HDL from an anti-inflammatory carrier into a dysfunctional, pro-inflammatory carrier rich in complement proteins.How does ApoE2 trigger drusen formation via phase separation?
The high-risk Apolipoprotein E2 (ApoE2) isoform triggers drusen formation through a cascade of metabolic dysfunction and physical phase changes. The retinal pigment epithelium (RPE) is the primary source of ApoE in the retina. In individuals with the ApoE2 isoform, inefficient intracellular cholesterol transport leads to a buildup of ceramides within the RPE, which causes autophagic dysfunction and complement-mediated mitochondrial damage.
Under this state of localized oxidative stress, reactive cysteines located at positions 112 and 158 of the ApoE2 protein undergo thiol oxidation. This specific oxidation event triggers liquid-liquid phase separation (LLPS), causing the proteins to assemble into biomolecular condensates.
Once formed, these condensates act as physical templates that catch and trap circulating blood-derived lipids, other apolipoproteins, and immunologic effectors. The accumulation of these trapped systemic components ultimately drives the nucleation and physical growth of drusen deposits in the space beneath the RP.
By contrast, the protective ApoE4 isoform lacks these reactive cysteines, which makes it resistant to phase separation and helps protect the sub-RPE space from this type of lipid and protein deposition.
Explain the "Meet, Greet, and Stick" hypothesis of drusenogenesis.
The "Meet, Greet, and Stick" hypothesis of drusenogenesis proposes that the primary building blocks of drusen—the hallmark extracellular deposits of early-to-intermediate age-related macular degeneration (AMD)—originate from the systemic bloodstream rather than being synthesized locally within the eye.
This hypothesis is supported by the following key mechanisms and findings:
- Systemic Origins: Comprehensive "drusenomics" studies reveal that approximately 60% to 61% of the proteins found in human drusen uniquely originate from the systemic circulation. By contrast, only a minor fraction (around 9%) is uniquely derived from local synthesis by the retinal pigment epithelium (RPE) or photoreceptors.
- Key Blood Components: The specific systemic components that make up these deposits heavily include blood-derived lipids, albumin, and apolipoproteins, particularly ApoA1 and other protein groups tied to HDL, LDL, and VLDL metabolism.
- Vessel Leakage (The "Meet" and "Greet"): As the eye ages, choroidal blood vessels become increasingly resistive and the basal lamina of the RPE becomes compromised. This structural decline allows these blood-derived proteins and lipid metabolites to filter out of the choroidal vessels and enter the extracellular space adjacent to the RPE.
- Accumulation (The "Stick"): Once they filter out of the bloodstream, these circulating components accumulate and "stick" together to form large physical deposits between the RPE and Bruch's membrane. As discussed previously regarding the ApoE2 genetic variant, localized liquid-liquid phase separation (LLPS) creates biomolecular condensates that act as physical templates to effectively catch, trap, and bind these circulating systemic lipids and proteins, driving the nucleation and growth of the druse
What is the "Neuroprotective Replenishment Protocol" for late AMD?
The Neuroprotective Replenishment Protocol is a targeted clinical strategy for late-stage age-related macular degeneration (AMD) designed to counteract severe systemic amino acid depletion and local lipid stress. The protocol is divided into specific diagnostic monitoring and targeted therapeutic interventions:
Diagnostic Monitoring Clinicians are advised to order a comprehensive fasting Plasma Amino Acids Profile and a high-sensitivity, mass spectrometry-based Serum Ketone Panel to track levels of acetoacetate and 3-hydroxybutyrate. This testing identifies the severe depletion of essential and aromatic amino acids—such as valine, leucine, phenylalanine, tyrosine, and histidine—which starves the neural retina of the precursors needed to synthesize glutamate and glutamine. It also tracks elevated ketones, which serve as systemic indicators of retinal pigment epithelium (RPE) lipotoxicity and lysosomal failure.
Therapeutic Modulation To bypass systemic depletion and stabilize the retina, the protocol utilizes a clinical-grade amino acid replenishment formula. Key interventions include:
- Valine and Leucine: Replenishing these essential branched-chain amino acids provides the nitrogen donors necessary to support retinal glutamate synthesis and activate cytoprotective mTOR pathways.
- L-Serine: Oral supplementation at 400 mg/kg/day is used to reduce neurotoxic deoxysphingolipid levels and preserve photoreceptors.
- L-Histidine: Administered at an oral dose of 5000 mg/kg to prevent the stabilization of hypoxia-induced HIF-1α.
- Taurine: Taken as a dietary load (4%) or in drinking water (0.2 M) to upregulate retinal antioxidant defense enzymes, restore the RPE's lysosomal clearance capacity, and preserve photoreceptor outer segments
What does a high Serum Ketone Panel indicate?
A high result on a Serum Ketone Panel—specifically showing elevated levels of the ketone bodies acetoacetate and 3-hydroxybutyrate (β-HB)—acts as a systemic biomarker for late-stage age-related macular degeneration (AMD).
In the context of AMD progression, this massive elevation indicates localized outer-retinal distress, specifically severe lipotoxicity and lysosomal failure within the retinal pigment epithelium (RPE).
When the RPE experiences extreme oxidative stress, its cellular clearance machinery becomes overwhelmed and fails to process the daily load of lipid-rich waste (like photoreceptor outer segment disks), leading to a toxic buildup of lipid debris and lipofuscin in the sub-RPE space. To cope with this severe lipotoxicity and preserve its mitochondrial function, the RPE significantly upregulates fatty acid oxidation and ketogenesis. Extracellular β-HB then acts as a potent signaling molecule to induce antioxidant defense enzymes and suppress neuroinflammation to help maintain the blood-retinal barrier.
Therefore, rather than just indicating dietary changes, a ketogenic spike detected in the bloodstream of an AMD patient serves as a direct clinical indicator that the RPE is actively fighting severe metabolic stress and lipid accumulation,






References:
- Thee EF, Acar İE, Colijn JM, Meester-Smoor MA, Verzijden T, Baart SJ, et al. Systemic metabolomics in a framework of genetics and lifestyle in age-related macular degeneration. Metabolites. 2023;13(6):701. doi:10.3390/metabo13060701.\
- Bergen AA, Arya S, Devrieze S, de Jong E, Lengyel I, Hysi P, et al. On the origin of proteins in human drusen: The meet, greet and stick hypothesis. Prog Retin Eye Res. 2019;70:55-84. doi:10.1016/j.preteyeres.2018.12.003.
- Lee SH, Montague AA, Sanislo SR, Almeida DRP, Montague AA, et al. Multi-omics liquid biopsy identifies mitochondrial dysfunction in geographic atrophy and supports the longevity-associated metabolite alpha-ketoglutarate as a therapeutic strategy. medRxiv [Preprint]. 2026. doi:10.64898/2026.03.12.26347263.
- National Institutes of Health Clinical Center. Effect of Nutritional Supplement Alpha-ketoglutarate for Age-related Ocular Disease (Metabolic Eye Therapy). ClinicalTrials.gov identifier: NCT07269704.
- Rowan S, Jiang S, Kessel MH, Chang ML, Rowan S, et al. Gut-retina axis, low-glycemia diet, and dietary patterns in age-related macular degeneration features. PNAS. 2017;114(22):E4472-E4481. doi:10.1073/pnas.1702302114.
- Satyanarayana G, Kumpakha R, Papania J, Sellers J, Chrenek M, Handa JT, Datta S. Dietary serine protects the retinal pigmented epithelium by blunting reactive oxygen species in dry age-related macular degeneration. bioRxiv [Preprint]. 2026. doi:10.64898/2026.04.30.722030.
- Lee TJ, Santeford A, Pitts KM, Ripoll CV, Terao R, Guo Z, et al. Apolipoprotein M attenuates age-related macular degeneration phenotypes via sphingosine-1-phosphate signaling and lysosomal lipid catabolism. Nat Commun. 2025;16(1):5331. doi:10.1038/s41467-025-60830-1.
- Garg R, Karmakar E, DeBruin D, Prasad S, Naquin E, Brennan M, et al. BDH1-dependent ketone body metabolism maintains Müller cell homeostasis and retinal function. bioRxiv [Preprint]. 2025. doi:10.64898/2025.12.27.696636.
- Xu R, Ritz BK, Wang Y, Huang J, Zhao C, Gong K, et al. The retina and retinal pigment epithelium differ in nitrogen metabolism and are metabolically connected. J Biol Chem. 2020;295(8):2324-2335. doi:10.1074/jbc.RA119.011784.
- Zhu S, Xu R, Engel AL, Wang Y, McNeel R, Hurley JB, et al. Proline provides a nitrogen source in the retinal pigment epithelium to synthesize and export amino acids for the neural retina. J Biol Chem. 2023;299(11). doi:10.1016/j.jbc.2023.105341.
- Reyes-Reveles J, Dhingra A, Alexander D, Bragin A, Philp NJ, Boesze-Battaglia K. Phagocytosis-dependent ketogenesis in retinal pigment epithelium. J Biol Chem. 2017;292(19):8038-8047. doi:10.1074/jbc.M116.770784.
- Froger N, Lattin GR, Martínez-Vacas L, Jafri S, et al. Therapeutic effects of taurine and histidine supplementation in retinal diseases. Life. 2024;14(12):1566. doi:10.3390/life14121566.
- Wang W, Cole JT, Contrusciere L, Ola MS, et al. Branched-chain amino acids metabolism and their roles in retinopathy: From relevance to mechanism. Nutrients. 2023;15(9):2161. doi:10.3390/nu15092161.
- Cipriani V, Han L, Wellcome Trust, et al. Phenome-wide Mendelian randomisation study of age-related macular degeneration. eLife. 2023;12:e82546. doi:10.7554/eLife.82546.
- Lowy-Gallego A, et al. Efficacy and safety of giving oral serine (an amino acid) on the progression of structural and functional changes of the retina in people with MacTel type 2. ClinicalTrials.gov identifier: NCT07342439.
- LipoScience Inc. Clinical relevance of Nuclear Magnetic Resonance LipoProfile. Frontiers in Nuclear Medicine. 2022;2:960522.
{kind=link}
Leave a comment
This site is protected by hCaptcha and the hCaptcha Privacy Policy and Terms of Service apply.