Lifestyle Factors and Geographic Atrophy (GA) Progression in Age-Related Macular Degeneration (AMD)
1. Introduction: The Clinical and Pathophysiological Landscape of Geographic Atrophy
Geographic Atrophy (GA) represents the advanced, non-neovascular stage of age-related macular degeneration (AMD) and stands as a formidable public health challenge in the developed world. Affecting more than five million individuals globally, the prevalence of this condition increases exponentially with age, positioning it as a primary cause of irreversible blindness among the elderly population.1 The disease is characterized clinically by the development of sharply demarcated atrophic lesions within the macula, representing the terminal result of the degeneration of photoreceptors, the retinal pigment epithelium (RPE), and the underlying choriocapillaris.2
The pathophysiology of GA is complex and multifactorial, involving a confluence of genetic susceptibility, oxidative stress, chronic inflammation, and lipid metabolic dysregulation. Unlike the neovascular (wet) form of AMD, which is driven largely by vascular endothelial growth factor (VEGF) and is amenable to anti-VEGF intravitreal therapy, GA has historically lacked effective treatment options. The condition typically manifests initially in the perifoveal region, sparing the central fovea and preserving visual acuity in the early stages. However, the natural history of the disease is one of inexorable expansion; lesions coalesce and enlarge over time, eventually encroaching upon the foveal center.3 The rate of this enlargement is highly variable among patients, ranging from 0.53 to 2.6 mm²/year, and is influenced by a diverse array of factors including baseline lesion size, multifocality, and distinct genetic and environmental inputs.3
Recent advancements in understanding the kinetics of GA progression have emerged from rigorous post hoc analyses of the Age-Related Eye Disease Study 2 (AREDS2). These analyses have illuminated a critical divergence in the disease process, described as a "Tale of Two Stages," wherein the risk factors governing the incidence of GA differ significantly from those driving its enlargement.5 This report provides an exhaustive synthesis of these findings, focusing specifically on modifiable lifestyle factors—diet, alcohol consumption, and smoking—and their impact on the anatomical and functional progression of Geographic Atrophy.

2. Methodological Framework: The AREDS2 Analysis of Disease Progression
To contextualize the findings regarding lifestyle factors, it is essential to understand the methodological rigor employed in the AREDS2 post hoc analyses. The AREDS2 study was a multi-center, randomized, double-masked clinical trial involving participants aged 50 to 85 years, designed primarily to evaluate the efficacy of oral supplementation in preventing progression to advanced AMD.6
2.1 Imaging and Grading Protocols
The assessment of GA progression in the AREDS2 cohort relied on centralized grading of annual stereoscopic color fundus photographs. Graders utilized planimetry tools to measure the area of GA within the AREDS grid. For eyes with multifocal disease—where multiple distinct lesions are present—the areas were summed to produce a total GA area for the eye.8 This rigorous anatomical measurement allowed for the precise tracking of lesion growth over a mean follow-up period of approximately 3 to 4.4 years.6
A critical component of the analysis was the mathematical transformation of the raw data. GA lesions typically expand at a rate dependent on their baseline circumference; larger lesions tend to grow faster in absolute area than smaller ones. To mitigate this confounding factor and allow for a fairer comparison of growth rates across eyes with varying baseline disease severity, researchers applied a square root transformation to the GA area measurements.6 This transformation linearizes the growth rate, ensuring that the reported enlargement rates (expressed in mm/year rather than mm²/year) reflect biological differences rather than geometric artifacts of initial lesion size.9
2.2 Statistical Modeling
The primary statistical tool employed was mixed-model repeated-measures regression. This sophisticated approach accounts for the correlation between eyes in bilateral cases and the repeated measurements over time within the same subject. The models were adjusted for a comprehensive set of covariates, including:
● Demographic Factors: Age, sex, and education level.
● Systemic Factors: Smoking status and total calorie intake.
● Ocular Characteristics: Baseline square root of GA area, lesion configuration (solid vs. multifocal), bilaterality, and central involvement.6
This methodological framework provides a high degree of confidence in the associations identified, suggesting that the observed effects of lifestyle factors on GA progression are independent of baseline disease characteristics and other potential confounders.
3. The Paradigm Shift: A Tale of Two Stages
One of the most profound theoretical insights emerging from the AREDS2 data is the concept that the biological mechanisms driving the initiation of geographic atrophy are partially distinct from those driving its expansion. This "Tale of Two Stages" paradigm challenges the assumption that risk factors for disease onset are identical to those for disease progression.5
3.1 Divergence of Genetic Drivers
The distinction between onset and progression is perhaps most clearly illustrated by genetic risk factors. The CFH (Complement Factor H) gene, located on chromosome 1, is a major driver of AMD incidence. Variants in CFH significantly increase the risk of developing early AMD and progressing to late stages. However, once GA is established, the CFH genotype appears to have a minimal or inconsistent effect on the rate of lesion enlargement.5 In contrast, risk variants at the ARMS2/HTRA1 locus on chromosome 10 are associated with both an increased risk of developing GA and a significantly faster rate of enlargement.5 This genetic divergence implies that while complement dysregulation may be the primary spark that ignites the disease (incidence), other mechanisms—such as mitochondrial dysfunction or extracellular matrix remodeling associated with ARMS2/HTRA1—may be more influential in fueling the fire of expansion.5

3.2 Implications for Environmental Risk Factors
This divergence extends to environmental and lifestyle factors. As detailed in subsequent sections, dietary components such as fish intake, which are highly protective against the development of AMD, show little to no association with the rate of GA enlargement. Conversely, other dietary factors that have a weaker association with incidence appear to play a dominant role in slowing progression.5 Understanding this distinction is paramount for clinicians, as it necessitates stage-specific patient counseling. Recommendations valid for preventing AMD may not be sufficient or optimized for patients who have already developed GA and are striving to preserve their remaining retinal tissue.

4. Dietary Patterns and Geographic Atrophy Enlargement
The role of nutrition in AMD has been a subject of intense investigation, culminating in the analysis of the Alternative Mediterranean Diet (aMedi) index within the AREDS2 cohort. This research provides compelling evidence that adherence to a Mediterranean-style diet is significantly associated with slower GA enlargement, independent of genetic risk.8
4.1 The Mediterranean Diet: Overall Impact
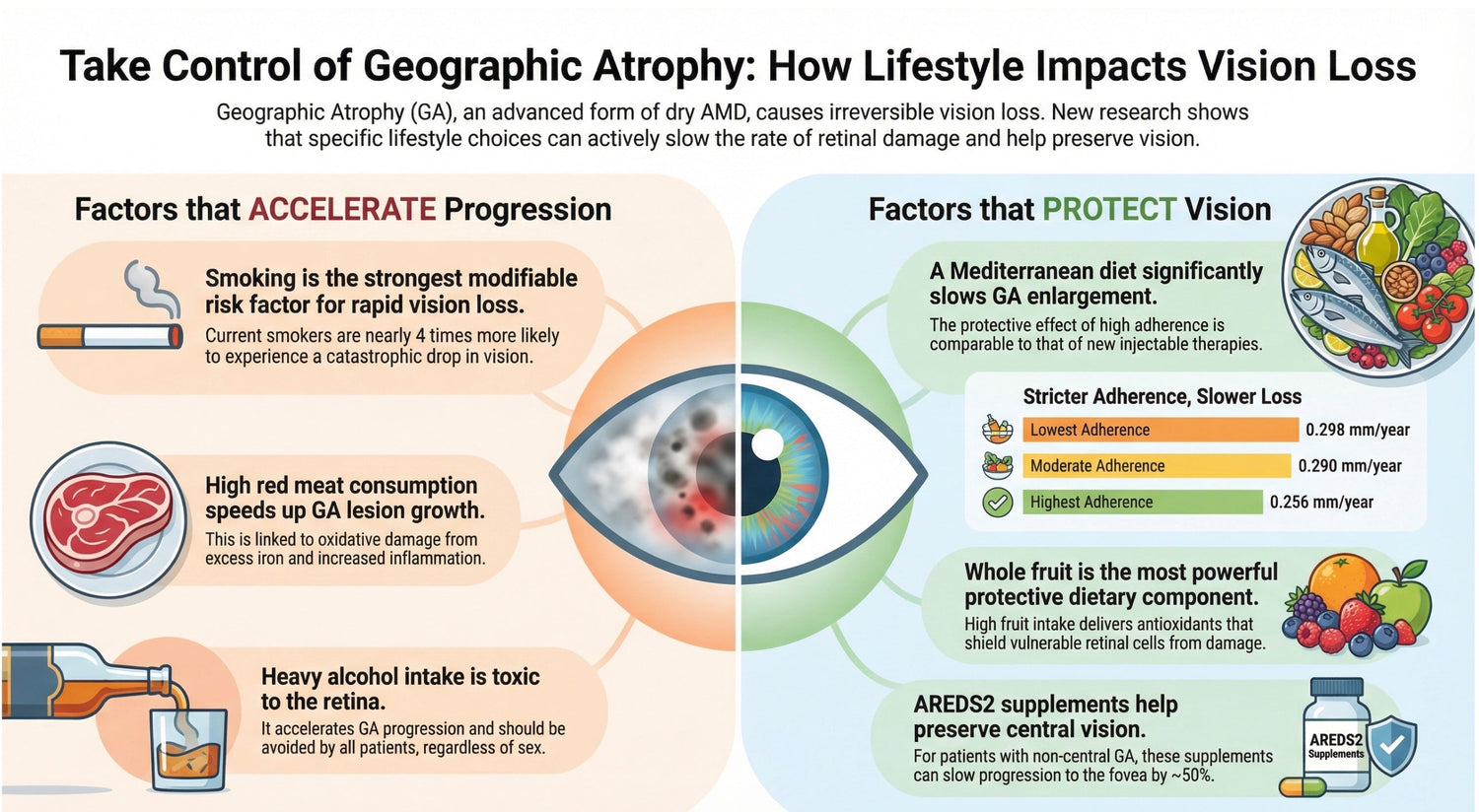
The Alternative Mediterranean Diet is characterized by high intakes of vegetables, fruits, nuts, whole grains, fish, and monounsaturated fats, coupled with moderate alcohol consumption and low intake of red meat. In the AREDS2 analysis, adherence to this dietary pattern demonstrated a statistically significant dose-response relationship with the rate of GA enlargement.8
Mixed-model regression analysis revealed that for each positive increment on the aMedi scale (ranging from 0 to 9), the rate of GA enlargement decreased by 0.007 mm/year (P = 0.019).8 While this numeric value may appear small, it represents a shift in the slope of progression that accumulates over years. When analyzed by tertiles of adherence, the difference becomes more clinically tangible. Patients in the highest tertile of adherence (scores 6-9) experienced significantly slower progression compared to those in the lowest tertile.
|
Adherence Level (aMedi Tertile) |
Mean GA Enlargement Rate (mm/year) |
95% Confidence Interval |
|
Tertile 1 (Lowest Adherence) |
0.298 |
0.280 – 0.317 |
|
Tertile 2 (Moderate Adherence) |
0.290 |
0.268 – 0.311 |
|
Tertile 3 (Highest Adherence) |
0.256 |
0.236 – 0.276 |
Table 1: Association between Mediterranean Diet Adherence and Geographic Atrophy Enlargement Rate. (Data source: 8)
The data indicate a clear protective trend: the stricter the adherence to the diet, the slower the expansion of the atrophic lesions. The difference of roughly 0.042 mm/year between the highest and lowest groups is statistically significant (P = 0.008 for trend) and suggests that dietary modification could function as a disease-modifying strategy.8
4.2 Component Analysis: The Protective Power of Whole Fruit
When the individual components of the Mediterranean diet were analyzed, whole fruit intake emerged as a dominant protective factor. The association was robust and highly significant (P = 0.0004), distinguishing fruit as a key driver of the overall diet's benefit.8
● Quantitative Findings: Patients in the highest quartile of fruit intake (≥14 servings/week for females, ≥12.5 servings/week for males) had a mean enlargement rate of 0.247 mm/year. In contrast, those in the lowest quartile (≤4 servings/week for females, ≤3 servings/week for males) progressed at a rate of 0.319 mm/year.8
● Mechanism: The biological plausibility of this finding lies in the high concentration of antioxidants, vitamins (C and E), and flavonoids present in whole fruits. The retina is a tissue with exceptionally high metabolic activity and oxygen consumption, making it uniquely vulnerable to oxidative stress. In GA, the "junctional zone" surrounding the atrophic lesion contains RPE cells that are under severe oxidative duress. The systemic delivery of fruit-derived antioxidants likely bolsters the defense mechanisms of these vulnerable cells, retarding the wave of apoptosis that drives lesion expansion.8 It is notable that the analysis specifically identified whole fruit, suggesting that the synergistic effect of fiber, fructose, and micronutrients in their natural matrix is superior to isolated components.8
4.3 Component Analysis: The Detrimental Role of Red Meat
Conversely, the consumption of red meat was identified as a significant risk factor for accelerated GA progression. The analysis revealed a strong positive association between red meat intake and the rate of lesion enlargement (P = 0.0002).8
● Quantitative Findings: Participants in the highest quartile of red meat consumption (≥5 servings/week for females, ≥7.5 servings/week for males) exhibited an enlargement rate of 0.312 mm/year. Those with lower intake levels showed significantly slower progression.8
● Mechanism: Several mechanisms may explain this deleterious effect. Red meat is a primary source of heme iron. While iron is essential for cellular function, excess iron can catalyze the Fenton reaction, generating highly reactive hydroxyl radicals that induce oxidative damage to the RPE and photoreceptors. Iron accumulation has been observed in Bruch's membrane and the RPE in AMD eyes, suggesting a direct toxic pathway. Additionally, red meat consumption is associated with systemic inflammation and the production of trimethylamine N-oxide (TMAO) by the gut microbiome, a metabolite linked to vascular endothelial dysfunction. Given the critical role of the choriocapillaris in GA, vascular impairment driven by a high-meat diet could exacerbate the ischemic component of the disease.8

4.4 The Fish Paradox: Incidence vs. Progression
A striking finding in the AREDS2 post hoc analysis is the lack of association between fish consumption and GA enlargement. While high intake of fatty fish (rich in omega-3 fatty acids DHA and EPA) is strongly associated with a reduced risk of developingAMD (incidence), it does not appear to significantly influence the rate at which GA lesions expand once they are present.11
● Statistical Findings: The P-value for the association between fish intake and GA enlargement was 0.14, indicating no statistical significance.8
● Implication: This "Fish Paradox" reinforces the "Tale of Two Stages" hypothesis. It suggests that the lipid membrane fluidity and anti-inflammatory properties conferred by omega-3s are critical for preventing the initial drusen formation and RPE dysfunction. However, once the threshold of atrophy is crossed, the disease process may become dominated by mechanisms (such as massive oxidative stress) that are less responsive to omega-3 modulation and more responsive to the antioxidant load provided by fruit.10

4.5 Other Dietary Components
The analysis of other Mediterranean diet components yielded mixed results.
● MUFA:SFA Ratio: A higher ratio of monounsaturated fatty acids (MUFA) to saturated fatty acids (SFA) was significantly associated with slower enlargement (P = 0.040). This supports the concept that healthy fats (like olive oil) are beneficial, likely through vascular protection of the choriocapillaris.8
● Vegetables: While vegetable intake is protective against AMD incidence, its association with GA enlargement did not reach statistical significance in the multivariate models (P = 0.24), although the trend was in the protective direction.8
● Legumes, Nuts, and Whole Grains: None of these components showed a statistically significant individual association with GA enlargement rates.8
5. Alcohol Consumption: A Sex-Stratified Analysis
The relationship between alcohol consumption and AMD progression is nuanced and exhibits distinct sexual dimorphism. The AREDS2 Report 34 provides a detailed examination of this relationship, challenging the simplistic "avoid all alcohol" or "alcohol is healthy" narratives by stratifying risk based on sex and consumption levels.13
5.1 General Epidemiological Context
Historically, heavy alcohol consumption has been linked to oxidative stress and nutritional depletion, both of which are detrimental to retinal health. However, moderate consumption has often been associated with cardiovascular benefits, leading to the hypothesis that it might benefit the ocular vasculature. The AREDS2 data clarifies these competing effects specifically for GA progression.15
5.2 Findings in Men: The U-Shaped Curve
In male participants, the relationship between alcohol intake and GA progression followed a pattern consistent with a protective effect at moderate levels.
● Moderate Consumption: Men who consumed moderate amounts of alcohol (defined as up to 3 standard drinks per day or 10-15g/day) demonstrated a decreased risk of progression to late AMD and a slower rate of GA enlargement compared to non-drinkers.13 The hazard ratio for progression to late AMD was 0.69 for low-to-moderate drinkers, indicating a substantial protective association.14
● Heavy Consumption: This protective effect disappeared or reversed at high levels of consumption. Heavy drinking was associated with accelerated GA progression and increased risk of early AMD.14
● Interpretation: For men, moderate alcohol intake appears to exert a beneficial effect, possibly due to hormetic mechanisms, antioxidant properties of specific beverages (e.g., polyphenols in wine), or improvements in choroidal perfusion. However, the threshold is critical; exceeding moderate limits introduces toxicity that outweighs any potential vascular benefit.13
5.3 Findings in Women: A Different Trajectory
The protective association observed in men was not consistently replicated in women.
● Progression Rates: Baseline GA progression rates were found to be faster in women (0.295 mm/year) compared to men (0.260 mm/year).14
● Alcohol Association: In women, the association between alcohol and disease progression was weaker and lacked the clear protective signal seen in men. Some data suggested a slight protective effect only at higher consumption levels, but the robust U-shaped benefit was absent.14
● Implication: This discrepancy suggests that biological differences in alcohol metabolism, body composition, or hormonal interactions influence how alcohol affects retinal pathology. Consequently, the potential "benefit" of moderate drinking cannot be universally recommended to female patients with the same confidence as for males.16
5.4 Public Health Recommendations
Despite the nuance regarding moderate intake in men, the overarching signal regarding heavy consumption is clear. Heavy alcohol intake is a risk factor for early AMD and accelerates GA progression. The authors of the AREDS2 report explicitly conclude that individuals with GA should avoid high alcohol consumption, regardless of sex.13

6. Cigarette Smoking: The Unambiguous Accelerator
While diet and alcohol show complex, variable associations, cigarette smoking remains the most consistent and potent modifiable risk factor for the progression of age-related macular degeneration.
6.1 Impact on Anatomical and Functional Progression
The deleterious effects of smoking on the retina are mediated through multiple pathways, including systemic oxidative stress, reduction of macular pigment density (lutein/zeaxanthin), and direct vasoconstriction of the choroidal blood supply.
● Anatomical Enlargement: In the AREDS2 mixed-model analysis, smoking status (current vs. never/former) was associated with faster GA enlargement. While some specific multivariate models adjusting for baseline size showed a borderline P-value (P = 0.05), the totality of evidence across AREDS reports consistently places smoking as a driver of lesion expansion.6
● Functional Decline: Crucially, smoking is a massive risk factor for rapid functional loss. In analyses identifying risk factors for a loss of 15 ETDRS letters (a doubling of the visual angle) within a single year, current smoking was identified as the strongest modifiable predictor. The adjusted odds ratio (aOR) for significant visual decline in smokers was 3.85.17This indicates that smokers are nearly four times more likely to experience a catastrophic drop in vision over a 12-month period compared to non-smokers.
6.2 Interaction with Genetics
The risk posed by smoking is further amplified by genetic susceptibility. Individuals with risk alleles at the ARMS2/HTRA1 or CFH loci who also smoke experience a synergistic increase in progression risk. Smoking essentially removes the environmental "buffer" that might otherwise protect a genetically susceptible retina, accelerating the onset of atrophy and the speed of its growth.5

7. Oral Micronutrient Supplementation: The Role of AREDS2 Formulation
The original AREDS and AREDS2 trials established the efficacy of antioxidant supplementation (Vitamin C, Vitamin E, Zinc, Copper, Lutein, Zeaxanthin) in preventing the conversion from intermediate to late AMD. However, the role of these supplements in patients who already have Geographic Atrophy has been a subject of debate. Recent analyses have clarified this role, specifically regarding the phenomenon of "foveal sparing".18
7.1 Extrafoveal vs. Foveal Lesions
Geographic atrophy lesions typically originate in the parafoveal belt (extrafoveal) and expand toward the center. The foveal RPE appears to have an intrinsic resistance to atrophy, a phenomenon known as foveal sparing.
● Supplement Efficacy: Post hoc analyses revealed that while AREDS2 supplements may not dramatically reduce the total area growth rate of the lesion (i.e., its expansion into the periphery), they significantly impact its progression toward the fovea. For patients with extrafoveal GA, oral supplementation was found to slow the rate of progression to the fovea by approximately 50%.18
● Mechanism: This finding suggests that the supplements augment the natural resilience of the fovea. The fovea contains the highest density of macular pigment (lutein and zeaxanthin). Supplementation likely saturates this reservoir, providing an enhanced antioxidant shield that delays the encroachment of the atrophic border into the visual center.18
7.2 Clinical Implication
This distinction is vital for patient counseling. Previously, patients with "dry AMD" (GA) might have been told that supplements offered no benefit once the advanced stage was reached. The new data indicates that for the specific subgroup of patients with non-central (extrafoveal) GA, continued supplementation is strongly indicated to preserve central vision for as long as possible.18

8. Functional Consequences: Visual Acuity and the "15-Letter Loss" Metric
Ultimately, the goal of managing GA progression is to preserve the patient's quality of life, which is inextricably linked to visual acuity. The anatomical enlargement of a lesion is only a proxy for the functional devastation it causes.
8.1 The Disconnect Between Anatomy and Function
A patient may harbor a large, multifocal GA lesion yet maintain 20/25 visual acuity if the foveal island is preserved. Conversely, a small lesion that breaches the foveal center can result in legal blindness (20/200). Therefore, identifying risk factors for rapid visual decline is as important as tracking lesion size.
● 15-Letter Loss: Regulatory agencies and clinical trials often use a loss of 15 ETDRS letters (3 lines) as a benchmark for clinically significant vision loss. In the AREDS2 cohort, approximately 5.5% of eyes with GA experienced this magnitude of loss within a single year.17

8.2 Risk Factors for Rapid Functional Decline
The analysis identified several independent risk factors for experiencing a ≥15-letter loss within one year:
1. Foveal Proximity: The strongest anatomical predictor. The closer the lesion is to the fovea, the higher the risk. For every 0.1 mm closer to the center, the odds of vision loss increased significantly (aOR 0.90, inverse relationship).17
2. Enlargement Rate: Eyes with faster-growing lesions are statistically more likely to overrun the fovea. An increase in enlargement rate of 0.1 mm/year raised the odds of vision loss by 12% (aOR 1.12).17
3. Baseline Acuity: Paradoxically, patients with worse baseline acuity (>20/40) were at higher risk of further rapid decline (aOR 2.09) compared to those with better vision. This likely reflects eyes that are already at the precipice of foveal failure.17
4. Genetics (CFH): While CFH mutations have a weaker influence on lesion area growth, they are a powerful risk factor for visual acuity loss. The presence of a CFH risk variant increased the odds of 15-letter loss by 4.63 times.17 This suggests that CFH-driven lesions may have a specific morphology or propensity for foveal involvement that is more destructive to central vision than lesions driven by other factors.
8.3 Diet and Visual Acuity
Adherence to the Mediterranean diet was also found to correlate with functional outcomes. In eyes with non-central GA, higher aMedi scores were associated with a slower decline in visual acuity. This functional protection mirrors the anatomical protection, confirming that the preservation of retinal tissue via diet translates directly to the preservation of sight.21

9. Genetic Underpinnings of Progression Rates
While lifestyle modifications offer a lever for patients to pull, the genetic architecture of the patient sets the baseline velocity of disease progression. Understanding the interplay between genetics and progression helps in stratifying risk.
9.1 The Role of ARMS2/HTRA1
As previously noted, variants in the ARMS2/HTRA1 region are unique in their ability to drive both incidence and progression. Patients homozygous for the risk allele at this locus typically exhibit a more aggressive disease phenotype, with faster enlargement rates and a higher likelihood of multifocality.5 This implies a distinct biological pathway—potentially related to mitochondrial bioenergetics—that remains active and damaging throughout the disease course.
9.2 The Role of Complement Genes (CFH, C3)
The complement pathway genes, particularly CFH and C3, are fundamental to the development of drusen and the initiation of atrophy. However, their impact on the rate of expansion is more complex. C3 risk variants have been associated with slower GA expansion in some analyses, highlighting the intricate feedback loops within the complement system.23 Conversely, CFHvariants, while less impactful on area growth, are strongly linked to functional visual loss, as detailed above.17
10. Clinical Implications and Patient Management
The findings from the AREDS2 post hoc analyses provide a robust evidence base for comprehensive patient counseling and management. The "watch and wait" approach to Geographic Atrophy is no longer tenable given the clear evidence that lifestyle factors can modify the disease trajectory.
10.1 Counseling Framework
Eye care professionals should integrate the following recommendations into the management plan for all GA patients:
|
Lifestyle Factor |
Recommendation |
Rationale |
|
Diet |
Adhere to Mediterranean Diet |
Slows GA area enlargement; preserves acuity. |
|
Fruit Intake |
Increase (>2 servings/day) |
Strongest dietary protector against enlargement. |
|
Red Meat |
Limit (<1 serving/week) |
Strongest dietary accelerator of enlargement. |
|
Smoking |
Cessation (Absolute) |
Prevents rapid visual decline (3.85x risk). |
|
Supplements |
AREDS2 Formula |
Slows progression to fovea in extrafoveal lesions. |
|
Alcohol |
Moderate (Men); Caution (Women) |
Moderate intake may be protective in men; heavy intake is toxic for all. |
Table 2: Clinical Counseling Summary for Geographic Atrophy Patients.
10.2 Integration with Emerging Therapies
The landscape of GA treatment is evolving with the approval of complement inhibitors (e.g., pegcetacoplan, avacincaptad pegol) that target C3 and C5. These drugs have been shown to reduce GA lesion growth by approximately 20-30% in clinical trials.24 It is notable that the magnitude of effect observed with high adherence to a Mediterranean diet (roughly a 22% reduction in growth rate between extreme quartiles) is comparable to the effect size of these pharmacological agents.8
This suggests that lifestyle modification should not be viewed as secondary to pharmacotherapy but rather as a foundational co-therapy. A synergistic approach—combining complement inhibition to dampen the immune drive with a high-antioxidant diet to mitigate oxidative stress—theoretically offers the maximal preservation of retinal tissue. Clinicians should emphasize that while injections treat the complement pathway, diet treats the metabolic environment of the RPE.25

10.3 Monitoring Protocols
Given the risks of rapid visual decline, monitoring protocols should be adjusted based on risk stratification. Patients with non-central lesions, smokers, or those with CFH mutations are at highest risk for sudden 15-letter loss and may warrant more frequent monitoring (e.g., every 4-6 months) with Fundus Autofluorescence (FAF) to track foveal proximity.17
11. Conclusion
The progression of Geographic Atrophy is not a monolithic or inevitable process determined solely by genetics. The detailed analyses of the AREDS2 cohort have illuminated a dynamic landscape where environmental inputs—specifically diet, smoking, and alcohol—actively shape the rate of retinal degeneration. The "Tale of Two Stages" paradigm clarifies that the tools required to slow progression (fruit, antioxidants, smoking cessation) are distinct from those used to prevent incidence (fish, omega-3s).
By adopting a Mediterranean-style diet rich in whole fruits and low in red meat, avoiding heavy alcohol consumption, and strictly abstaining from smoking, patients can significantly alter the slope of their disease progression. For those with extrafoveal lesions, AREDS2 supplementation provides a critical buffer for the fovea, extending the period of useful central vision. As we enter a new era of therapeutic intervention for GA, these lifestyle factors remain the bedrock of patient care, empowering individuals to take an active, effective role in the preservation of their sight. The evidence is clear: the environment within the eye is modifiable, and optimizing it is essential for checking the advance of this blinding disease.


Reference cited:
1. Geographic Atrophy | amdbook.org, accessed January 3, 2026, https://amdbook.org/content/geographic-atrophy-0
2. OCT risk factors for 2-year foveal involvement in non-treated eyes with extrafoveal geographic atrophy and AMD - PubMed Central, accessed January 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC11222248/
3. The Progression of Geographic Atrophy Secondary to Age-Related Macular Degeneration - OphEd, accessed January 3, 2026, https://www.ophed.com/system/files/2018/03/The%20Progression%20of%20%20Geographic%20Atrophy%20secondary%20to%20Age-Related%20Macular%20degeneration.pdf
4. Geographic Atrophy - The American Macular Degeneration Foundation, accessed January 3, 2026, https://www.macular.org/about-macular-degeneration/geographic-atrophy
5. Geographic Atrophy in Age-Related Macular Degeneration: A Tale of Two Stages - PubMed, accessed January 3, 2026, https://pubmed.ncbi.nlm.nih.gov/37197703/
6. Progression of Geographic Atrophy in Age-related Macular Degeneration: AREDS2 Report Number 16 - Houston Methodist Scholars, accessed January 3, 2026, https://scholars.houstonmethodist.org/en/publications/progression-of-geographic-atrophy-in-age-related-macular-degenera/
7. Progresssion of geographic atrophy in age-related macular ..., accessed January 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC6246813/
8. Adherence to a Mediterranean Diet and Geographic Atrophy ..., accessed January 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC9464676/
9. Progression of geographic atrophy with subsequent exudative neovascular disease in age-related macular degeneration: AREDS2 Report 24 - PubMed Central, accessed January 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC7870515/
10. Adherence to a Mediterranean Diet and Geographic Atrophy Enlargement Rate in the Age-Related Eye Disease Study 2: AREDS2 Report 28 | Request PDF - ResearchGate, accessed January 3, 2026, https://www.researchgate.net/publication/359716349_Adherence_to_a_Mediterranean_Diet_and_Geographic_Atrophy_Enlargement_Rate_in_the_Age-Related_Eye_Disease_Study_2_AREDS2_Report_28
11. Relationships Between Diet and Geographic Atrophy Progression in the Age-Related Eye Diseases Studies 1 and 2 - MDPI, accessed January 3, 2026, https://www.mdpi.com/2072-6643/17/5/771
12. Relationships Between Diet and Geographic Atrophy Progression in the Age-Related Eye Diseases Studies 1 and 2 - PubMed, accessed January 3, 2026, https://pubmed.ncbi.nlm.nih.gov/40077641/
13. Alcohol Consumption and Risk of Age-Related Macular Degeneration and Geographic Atrophy Progression: Age-Related Eye Diseases Study 2 Report 34 - PubMed, accessed January 3, 2026, https://pubmed.ncbi.nlm.nih.gov/39547357/
14. Study links alcohol consumption to AMD and GA progression patterns - Ophthalmology 360, accessed January 3, 2026, https://ophthalmology360.com/geographic-atrophy/study-links-alcohol-consumption-to-amd-and-ga-progression-patterns/
15. Alcohol consumption and the risk of age-related macular degeneration: a systematic review and meta-analysis - PubMed, accessed January 3, 2026, https://pubmed.ncbi.nlm.nih.gov/18242575/
16. Eye Disease Progression: The Effects of Alcohol Consumption in Women and Men - Peer to Peer: Spotlight on AMD - MedPage Today, accessed January 3, 2026, https://www.medpagetoday.com/resource-centers/peer-to-peer-spotlight-amd/eye-disease-progression-effects-alcohol-consumption-women-and-men/5602
17. Rapid Visual Decline in Geographic Atrophy May Be Influenced by Several Factors, accessed January 3, 2026, https://www.aao.org/education/editors-choice/rapid-visual-decline-in-geographic-atrophy-may-be-
18. A new era of oral supplements for geographic atrophy?, accessed January 3, 2026, https://www.retina-specialist.com/article/a-new-era-of-oral-supplements-for-geographic-atrophy
19. Associations between Dietary Nutrient Intake and Geographic Atrophy Progression towards the Central Macula | IOVS, accessed January 3, 2026, https://iovs.arvojournals.org/article.aspx?articleid=2793847
20. Risk Factors for 15-Letter Visual Acuity Loss from Geographic Atrophy Progression over 1 Year in the Age-Related Eye Disease Study 2 - PubMed, accessed January 3, 2026, https://pubmed.ncbi.nlm.nih.gov/40939951/
21. Relationships Between Diet and Geographic Atrophy Progression in the Age-Related Eye Diseases Studies 1 and 2 - PubMed Central, accessed January 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC11901604/
22. Relationships Between Diet and Geographic Atrophy Progression in the Age-Related Eye Diseases Studies 1 and 2 - Semantic Scholar, accessed January 3, 2026, https://www.semanticscholar.org/paper/Relationships-Between-Diet-and-Geographic-Atrophy-1-Agr%C3%B3n-Vance/23903bd4e30d0bb73ebd6f3f24542e50606ac712
23. Alcohol Consumption and Risk of Age-Related Macular Degeneration and Geographic Atrophy Progression: AREDS2 Report 34 | Request PDF - ResearchGate, accessed January 3, 2026, https://www.researchgate.net/publication/385836385_Alcohol_Consumption_and_Risk_of_Age-Related_Macular_Degeneration_and_Geographic_Atrophy_Progression_AREDS2_Report_34?_tp=eyJjb250ZXh0Ijp7InBhZ2UiOiJzY2llbnRpZmljQ29udHJpYnV0aW9ucyIsInByZXZpb3VzUGFnZSI6bnVsbCwic3ViUGFnZSI6bnVsbH19
24. Geographic atrophy: pathophysiology and current therapeutic strategies - PMC, accessed January 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC11182118/
25. Diet and ideal food pyramid to prevent or support the treatment of diabetic retinopathy, age-related macular degeneration, and cataracts - PMC - PubMed Central, accessed January 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC10265999/
{kind=link}
Leave a comment
This site is protected by hCaptcha and the hCaptcha Privacy Policy and Terms of Service apply.