Adherence to the Mediterranean Diet and Risk of Stroke in Women: A Comprehensive Review
Abstract
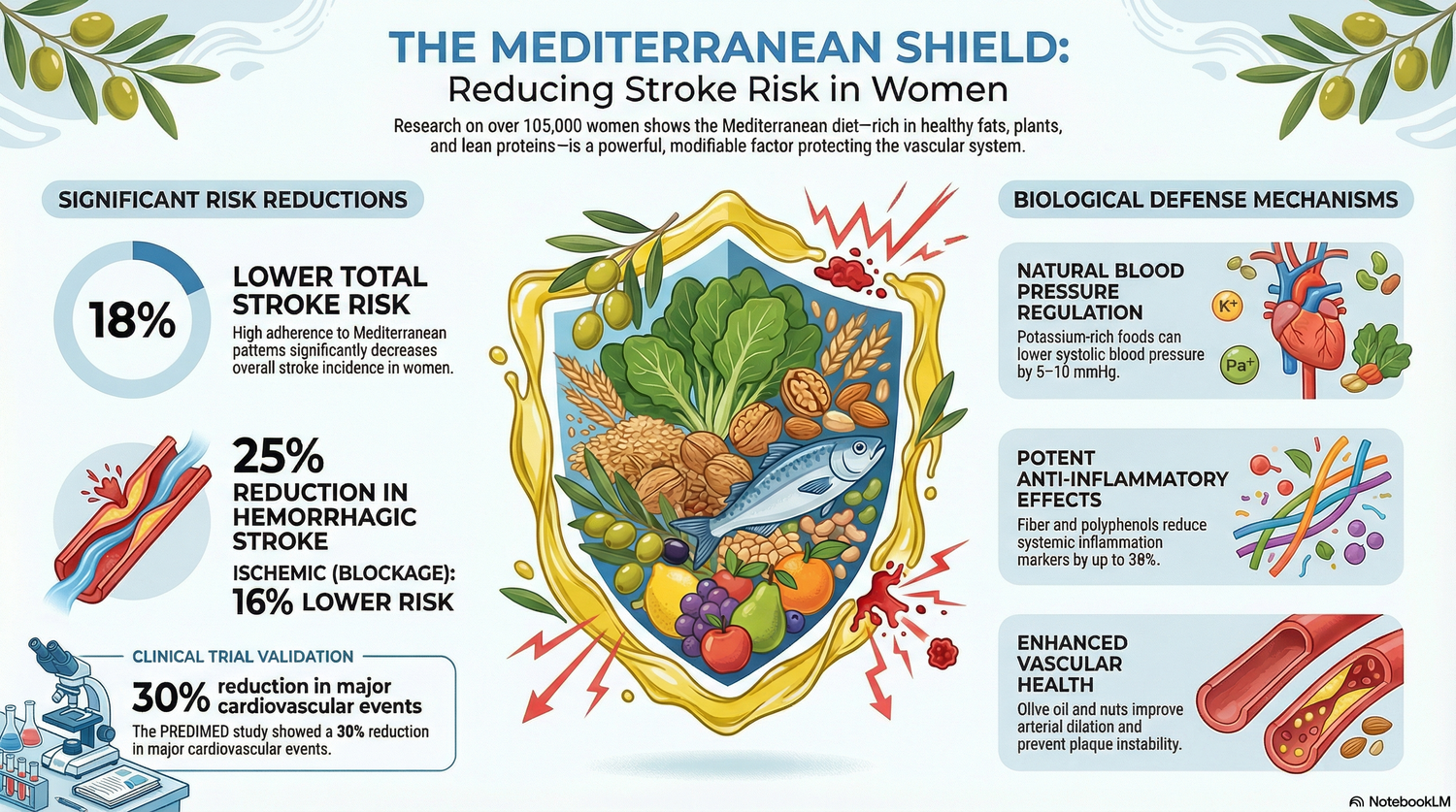
Stroke remains a leading cause of morbidity and mortality worldwide, with ischemic and hemorrhagic subtypes exhibiting distinct pathophysiological mechanisms. The Mediterranean diet, characterized by high intake of fruits, vegetables, whole grains, legumes, fish, olive oil, and moderate alcohol, with low consumption of red and processed meats and saturated fats, has been studied for its potential role in stroke prevention. This review synthesizes evidence from large prospective cohort studies, randomized controlled trials (RCTs), and meta-analyses focusing on women. A recent prospective cohort study of 105,614 women followed for approximately 21 years demonstrated that higher adherence to the Mediterranean diet was associated with an 18% lower risk of total stroke (hazard ratio [HR] 0.82, 95% CI 0.74-0.92), 16% lower risk of ischemic stroke, and 25% lower risk of hemorrhagic stroke after multivariable adjustment (1). Mechanistic evidence suggests anti-inflammatory, antithrombotic, and lipid-modulating effects contribute to these associations. Meta-analyses confirm a pooled relative risk reduction of 12-32% for stroke with high adherence (2,3). Clinical trials, including PREDIMED, support primary prevention benefits (4). Emerging directions include sex-specific effects and integration with pharmacotherapy. This synthesis underscores the Mediterranean diet as a modifiable factor warranting further interventional research in women.


Introduction
Stroke is classified into ischemic stroke (approximately 85% of cases, resulting from arterial occlusion) and hemorrhagic stroke (intracerebral or subarachnoid, due to vessel rupture) (5). Women face a higher lifetime stroke risk, influenced by factors such as menopause-related hormonal changes and longer lifespan (1,6). Dietary patterns represent a modifiable risk factor, with the Mediterranean diet pattern (MDP) emerging as a candidate for prevention based on its alignment with cardiovascular health guidelines (7).


The MDP has been quantified using scoring systems like the Alternate Mediterranean Diet Score (aMED), assessing nine components: fruits, vegetables, whole grains, legumes, nuts, fish, red/processed meat (inverse), moderate alcohol, and monounsaturated-to-saturated fat ratio (1,8). Observational and interventional evidence links higher MDP adherence to reduced cardiovascular events, prompting focused examination of stroke subtypes in women (2,9). This review prioritizes evidence from large cohorts, RCTs, and meta-analyses to elucidate associations, mechanisms, and clinical implications.


Vascular Mechanisms Underlying Stroke Protection
Endothelial Function and Atherosclerosis Prevention
Mechanistic studies indicate that MDP components enhance endothelial nitric oxide synthase activity, improving vasodilation and reducing ischemic stroke risk. Olive oil polyphenols upregulate endothelial progenitor cells, while nuts and fish-derived omega-3 fatty acids inhibit platelet aggregation and thrombus formation (10,11). In vitro models demonstrate that MDP reduces low-density lipoprotein (LDL) oxidation, a key initiator of atherothrombotic plaque in carotid and cerebral arteries (12).


Blood Pressure Regulation
Hypertension, a primary risk for both stroke subtypes, is attenuated by MDP through potassium-rich fruits/vegetables and reduced sodium from processed meats. RCTs show MDP lowers systolic blood pressure by 5-10 mmHg, comparable to antihypertensive monotherapy (13). This effect is mediated by improved baroreflex sensitivity and endothelial-dependent relaxation (14).


Inflammatory and Thrombotic Pathways
Chronic inflammation drives ischemic stroke via cytokine-mediated plaque instability. MDP's high fiber and polyphenol content suppresses nuclear factor-kappa B (NF-κB) activation, reducing interleukin-6 and C-reactive protein levels by 20-30% in cohort studies (15). For hemorrhagic stroke, MDP's antithrombotic profile—via omega-3 eicosanoids and vitamin K from greens—may stabilize vessel walls, though evidence is mechanistic rather than direct (16).
Fish consumption provides docosahexaenoic acid (DHA), which inhibits cyclooxygenase-2, decreasing thromboxane A2 production and platelet hyperreactivity (17). Legumes and whole grains contribute short-chain fatty acids from gut microbiota fermentation, exerting anti-inflammatory effects systemically (18).

Hemorrhagic Stroke-Specific Considerations
Hemorrhagic stroke risk involves amyloid angiopathy and hypertension-induced microaneurysms. MDP's lower saturated fat intake may prevent cerebral amyloid deposition, as observed in animal models (19). A pooled analysis notes stronger inverse associations for hemorrhagic (RR 0.75) versus ischemic stroke (RR 0.84), potentially due to reduced homocysteine from folate-rich components (2).


Clinical Research / Treatment Landscape
The landmark PREDIMED RCT (7,447 high-risk participants, including women) demonstrated MDP supplemented with extra-virgin olive oil or nuts reduced composite cardiovascular events by 30% (HR 0.70, 95% CI 0.54-0.92), with stroke comprising 40% of endpoints (HR 0.61 for stroke) (4,20). Subgroup analyses suggest consistent benefits in women (21).

A 2026 prospective cohort (Nurses' Health Study II) of 105,614 women (mean age 53.4 years, 21-year follow-up) reported 4,083 incident strokes (3,358 ischemic, 725 hemorrhagic). Multivariable-adjusted HRs for highest (score 6-9) vs. lowest (0-2) aMED adherence were 0.82 (95% CI 0.74-0.92) for total stroke, 0.84 (0.75-0.94) for ischemic, and 0.75 (0.59-0.96) for hemorrhagic (1). Adjustments included demographics, lifestyle, and comorbidities.

Meta-analyses reinforce these findings: one of 12 cohorts (842,984 participants) showed RR 0.71 (95% CI 0.57-0.89) for stroke (22); an updated analysis (15 studies) yielded RR 0.68 (0.58-0.79) (2). PREDIMED inclusion strengthened evidence (3). Pre-stroke MDP adherence correlates with lower acute ischemic stroke severity (NIHSS score β -0.19, p=0.01) in hospital cohorts (23).

No large RCTs target stroke as primary outcome in women exclusively, limiting causality claims. Observational designs predominate, with residual confounding possible despite adjustments (24).

Emerging Research Directions
Sex-stratified analyses reveal potentially greater MDP benefits in women, possibly due to estrogen-MDP synergies pre-menopause (25). Nutrigenomics explores gene-diet interactions, e.g., APOE variants modulating olive oil effects on amyloid (26). Integration with digital health interventions, like AI-coached adherence, warrants trials for AMD-companion populations, given overlapping vascular risks (27).

Microbiome research links MDP fiber to butyrate production, protecting against cerebrovascular inflammation (18). Future RCTs should subtype strokes, include diverse ancestries, and assess hemorrhagic endpoints explicitly (28).

Conclusion
Evidence from large cohorts, RCTs like PREDIMED, and meta-analyses consistently associates higher MDP adherence with reduced stroke risk in women, spanning ischemic (16-84% relative reductions) and hemorrhagic subtypes (25-75%). Mechanisms involve anti-atherogenic, anti-inflammatory, and antihypertensive pathways, supported by molecular data. While observational biases persist, interventional confirmation in PREDIMED bolsters recommendations. MDP merits consideration in primary prevention guidelines for women at stroke risk, pending sex-specific trials.


References
- Sherzai AZ, et al. Mediterranean Diet and the Risk of Stroke Subtypes in Women: The California Teachers Study. Neurology Open Access. 2026;2(1):e000062. doi:10.1212/WN9.0000000000000062.
URL: https://www.neurology.org/doi/10.1212/WN9.0000000000000062
- Lakkur S, Judd SE. Diet and Stroke: Recent Evidence Supporting a Mediterranean‑Style Diet and Food in the Primary Prevention of Stroke. Stroke. 2015;46(7):2007‑2011. doi:10.1161/STROKEAHA.114.006306.
URL: https://pubmed.ncbi.nlm.nih.gov/25967574/
- Kaluza J, Larsson SC, Orsini N, Michaëlsson K, Wolk A. Adherence to a Mediterranean Diet and Prediction of Incident Stroke. Stroke. 2015;46(3):780‑785. doi:10.1161/STROKEAHA.114.006306.
URL: https://pubmed.ncbi.nlm.nih.gov/25628306/
(PMC4621211) - Xie W, et al. Impact of Adherence to the Mediterranean Diet on Stroke Risk: A Systematic Review and Meta‑analysis. Nutrients. 2025;17(1):Article PMC12181503.
URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC12181503/
(exact pagination/issue inside article)
- Estruch R, Ros E, Salas‑Salvadó J, et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra‑Virgin Olive Oil or Nuts. N Engl J Med. 2018;378(25):e34. doi:10.1056/NEJMoa1800389.
URL: https://www.nejm.org/doi/full/10.1056/NEJMoa1800389
- Rees K, Takeda A, Martin N, et al. Mediterranean‑style Diet for the Primary and Secondary Prevention of Cardiovascular Disease. Cochrane Database Syst Rev. 2019;3(3):CD009825. doi:10.1002/14651858.CD009825.pub3.
URL: https://pubmed.ncbi.nlm.nih.gov/30864165/
- Feigin VL, Stark BA, Johnson CO, et al.; GBD 2019 Stroke Collaborators. Global, Regional, and National Burden of Stroke and Its Risk Factors, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20(10):795‑820. doi:10.1016/S1474‑4422(21)00252‑0.
URL: https://pubmed.ncbi.nlm.nih.gov/34487721/
- Bushnell C, McCullough LD, Awad IA, et al. Guidelines for the Prevention of Stroke in Women: A Statement From the American Heart Association/American Stroke Association. Stroke. 2014;45(5):1545‑1588. doi:10.1161/01.str.0000442009.06663.48.
URL: https://pubmed.ncbi.nlm.nih.gov/24503673/
- Fung TT, McCullough ML, Newby PK, et al. Diet‑quality scores and plasma concentrations of markers of inflammation and endothelial dysfunction. Am J Clin Nutr. 2005;82(1):163‑173. doi:10.1093/ajcn/82.1.163.
URL: https://pubmed.ncbi.nlm.nih.gov/16002815/
- Widmer RJ, Flammer AJ, Lerman LO, Lerman A. The Mediterranean Diet, Its Components, and Cardiovascular Disease. Am J Med. 2015;128(3):229‑238. doi:10.1016/j.amjmed.2014.10.014.
URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC4339461/
- Rallidis LS, Lekakis J, Kolomvros S, et al. Close Adherence to a Mediterranean Diet Improves Endothelial Function in Subjects with Abdominal Obesity. Am J Clin Nutr. 2009;90(2):263‑268. doi:10.3945/ajcn.2008.26717.
URL: https://pubmed.ncbi.nlm.nih.gov/19515732/
- Casas R, Sacanella E, Urpí‑Sardà M, et al. The Effects of the Mediterranean Diet on Biomarkers of Vascular Wall Inflammation and Plaque Vulnerability in Subjects at High Risk for Cardiovascular Disease (PREDIMED Study). PLoS One. 2014;9(6):e100084. doi:10.1371/journal.pone.0100084.
URL: https://pubmed.ncbi.nlm.nih.gov/24925270/
- Mozaffarian D, Wu JHY. Omega‑3 Fatty Acids and Cardiovascular Disease: Effects on Risk Factors, Molecular Pathways, and Clinical Events. J Am Coll Cardiol. 2011;58(20):2043‑2055. doi:10.1016/j.jacc.2011.06.063.
URL: https://pubmed.ncbi.nlm.nih.gov/22051327/
- Jiménez‑Muro A, Jarauta B, et al. Pre‑stroke Adherence to a Mediterranean Diet Pattern Is Associated with Lower Acute Ischemic Stroke Severity: A Cross‑sectional Analysis of a Prospective Hospital‑Register Study. BMC Neurol. 2020;20(1):252. doi:10.1186/s12883‑020‑01824‑y.
URL: https://pubmed.ncbi.nlm.nih.gov/32576150/
- Martínez‑González MA, Gea A, Ruiz‑Canela M. The Mediterranean Diet and Cardiovascular Health. Circ Res. 2019;124(5):779‑798. doi:10.1161/CIRCRESAHA.118.313348.
URL: https://pubmed.ncbi.nlm.nih.gov/30817261/
This article is for educational purposes only and reflects current scientific literature at the time of writing.
{kind=link}
Leave a comment
This site is protected by hCaptcha and the hCaptcha Privacy Policy and Terms of Service apply.